Korean J Sports Med.
2014 Dec;32(2):133-138. 10.5763/kjsm.2014.32.2.133.
Arthroscopic Biceps Tenodesis: Soft Tissue versus Bone Fixation
- Affiliations
-
- 1Department of Orthopedic Surgery, Gil Hospital, Gachon University, Incheon, Korea. jjangumom52@hanmail.net
- KMID: 2288670
- DOI: http://doi.org/10.5763/kjsm.2014.32.2.133
Abstract
- The purpose of our study was to compare the clinical results between arthroscopic bone fixation on intertubercular groove using suture anchor and soft tissue fixation at the rotaor interval for biceps tenodesis when partial tear or instability of biceps tendon accompanied with rotator cuff tear. From January 2010 to January 2012, 34 cases who were performed biceps tenodesis for partial tear or instability were enrolled in our study. Mean follow-up period was 30.2 months. Bone fixation using suture anchor was performed in 18 cases, and soft tissue fixation was performed in 16 cases. Clinical result was evaluated by pain visual analogue scale (VAS), Speed test, Yergason test, muscle strength, and Constant score. Pain VAS of cases with soft tissue fixation was significantly higher than that of cases with bone fixation at 6 months and final follow-up. Positive results for the final follow-up Speed and Yergason test were checked in 4 cases (25%) with soft tissue fixation and 1 (5.6%) with bone fixation. The Popeye deformity was seen in 4 cases (25%) with soft tissue fixation and 2 (11%) with bone fixation. Constant score was improved 47 to 78 in cases with soft tissue fixation and 48 to 86 in cases with bone fixation. In patient with partial tear or instability of biceps tendon accompanied with rotator cuff tear, biceps tenodesis using soft tissue fixation showed worse result compared with bone fixation because of long duration of the pain. Therefore, when performing the biceps tenodesis, bone fixation will be recommended.
MeSH Terms
Figure
-

Fig. 1. (A) This is an illustration figure of bony tenodesis and there are 2 strands through the biceps tendon like Z shape. There are arthroscopic findings of bony tenodesis after passing (B) and tying (C) the biceps tendon with non-absorbable sutures.
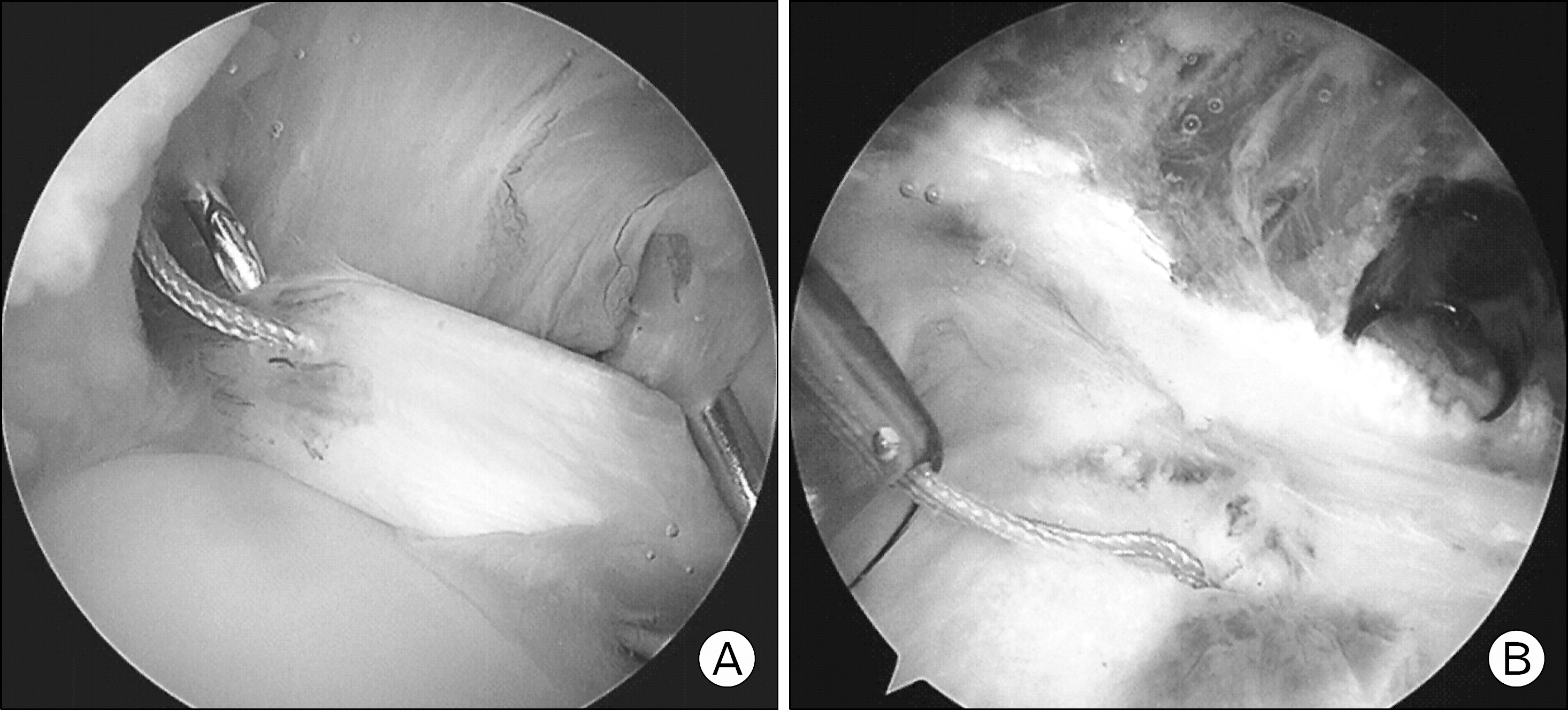
Fig. 2. There are arthroscopic findings of soft tissue tenodesis after passing (A) and tying (B) the biceps tendon with non-ab-sorbable sutures.
Reference
-
1. Hitchcock HH, Bechtol CO. Painful shoulder; observations on the role of the tendon of the long head of the biceps brachii in its causation. J Bone Joint Surg Am. 1948; 30:263–73.2. Froimson AI, O I. Keyhole tenodesis of biceps origin at the shoulder. Clin Orthop Relat Res. 1975; 112:245–9.
Article3. Mariani EM, Cofield RH, Askew LJ, Li GP, Chao EY. Rupture of the tendon of the long head of the biceps brachii. Surgical versus nonsurgical treatment. Clin Orthop Relat Res. 1988; 228:233–9.4. Gartsman GM, Hammerman SM. Arthroscopic biceps tenodesis: operative technique. Arthroscopy. 2000; 16:550–2.
Article5. Boileau P, Krishnan SG, Coste JS, Walch G. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002; 18:1002–12.
Article6. Sekiya JK, Elkousy HA, Rodosky MW. Arthroscopic biceps tenodesis using the percutaneous intra-articular transtendon technique. Arthroscopy. 2003; 19:1137–41.
Article7. Elkousy H, Romero JA, Edwards TB, Gartsman GM, O'Connor DP. Ultrasound and clinical evaluation of soft-tissue versus hardware biceps tenodesis: is hardware tenodesis worth the cost? Am J Orthop (Belle Mead NJ). 2014; 43:62–5.8. Brandsma JW, Schreuders TA, Birke JA, Piefer A, Oosten-dorp R. Manual muscle strength testing: intraobserver and interobserver reliabilities for the intrinsic muscles of the hand. J Hand Ther. 1995; 8:185–90.
Article9. Paulos LE, Mendez KT, Berg T. A novel approach to arthroscopic biceps tenodesis. Oper Tech Sports Med. 2007; 15:27–34.
Article10. Kim YK, Kim DW, Lee JH. Long head of the biceps tendon lesion associated with rotator cuff tear. J Korean Shoulder Elbow Soc. 2010; 13:64–71.
Article11. Barber FA, Byrd JW, Wolf EM, Burkhart SS. How would you treat the partially torn biceps tendon? Arthroscopy. 2001; 17:636–9.
Article12. Boileau P, Baque F, Valerio L, Ahrens P, Chuinard C, Trojani C. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007; 89:747–57.
Article13. Wolf EM. A case for tenotomy of the long head of the biceps. Proceedings of the 22nd Annual Meeting Arthroscopy Association of North America; Phoenix (AZ):. 2003. 771–6.14. Frost A, Zafar MS, Maffulli N. Tenotomy versus tenodesis in the management of pathologic lesions of the tendon of the long head of the biceps brachii. Am J Sports Med. 2009; 37:828–33.
Article15. Romeo AA, Mazzocca AD, Tauro JC. Arthroscopic biceps tenodesis. Arthroscopy. 2004; 20:206–13.
Article16. Mazzocca AD, Romeo AA. Arthroscopic biceps tenodesis in the beach chair position. Operative Techniques in Sports Medicine. 2003; 11:6–14.
Article17. Mazzocca AD, Bicos J, Santangelo S, Romeo AA, Arciero RA. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005; 21:1296–306.
Article18. Levin SD, Wellman DS, Liu C, et al. Biomechanical strain characteristics of soft tissue biceps tenodesis and bony tenodesis. J Orthop Sci. 2013; 18:699–704.
Article19. Ahmed M, Young BT, Bledsoe G, Cutuk A, Kaar SG. Biomechanical comparison of long head of biceps tenodesis with interference screw and biceps sling soft tissue techniques. Arthroscopy. 2013; 29:1157–63.
Article20. Scheibel M, Schroder RJ, Chen J, Bartsch M. Arthroscopic soft tissue tenodesis versus bony fixation anchor tenodesis of the long head of the biceps tendon. Am J Sports Med. 2011; 39:1046–52.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Is the Strong Fixation Necessary in Performing Biceps Tenodesis?
- Clinical Results of Arthroscopic Biceps Long Head Tenodesis Above the Pectoralis Major Using an Interference Screw
- Short-Term Results of Subpectoral Tenodesis of the Proximal Biceps Tendon Using by Interference Screw
- Arthroscopic Tenotomy for Lesions of the Long Head of the Biceps Brachii
- Intraoperative periprosthetic humeral fracture during reverse shoulder arthroplasty: a sequelae of prior biceps tenodesis
