Robotic single-port transumbilical total hysterectomy: a pilot study
- Affiliations
-
- 1Women's Cancer Clinic, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Yonsei University College of Medicine, Seoul, Korea. ytkchoi@yuhs.ac
- KMID: 2288576
- DOI: http://doi.org/10.3802/jgo.2011.22.2.120
Abstract
OBJECTIVE
To evaluate the feasibility of robotic single-port transumbilical total hysterectomy using a home-made surgical glove port system.
METHODS
We retrospectively reviewed the medical records of patients who underwent robotic single-port transumbilical total hysterectomy between January 2010 and July 2010. All surgical procedures were performed through a single 3-4-cm umbilical incision, with a multi-channel system consisting of a wound retractor, a surgical glove, and two 10/12-mm and two 8 mm trocars.
RESULTS
Seven patients were treated with robotic single-port transumbilical total hysterectomy. Procedures included total hysterectomy due to benign gynecological disease (n=5), extra-fascial hysterectomy due to carcinoma in situ of the cervix (n=1), and radical hysterectomy due to cervical cancer IB1 (n=1). The median total operative time was 109 minutes (range, 105 to 311 minutes), the median blood loss was 100 mL (range, 10 to 750 mL), and the median weight of the resected uteri was 200 g (range, 40 to 310 g). One benign case was converted to 3-port robotic surgery due to severe pelvic adhesions, and no post-operative complications occurred.
CONCLUSION
Robotic single-port transumbilical total hysterectomy is technically feasible in selected patients with gynecological disease. Robotics may enhance surgical skills during single-port transumbilical hysterectomy, especially in patients with gynecologic cancers.
Keyword
MeSH Terms
Figure
-
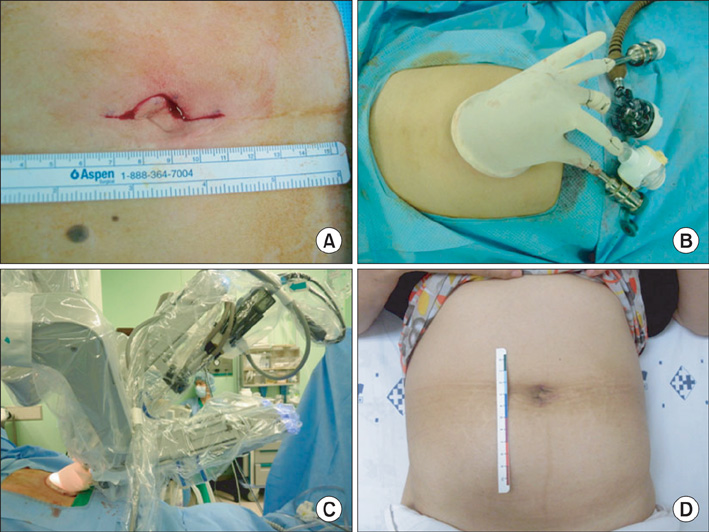
Fig. 1 Photograph demonstrating a robotic single-port transumbilical access system. (A) A 3-4 cm vertical transumbilical skin incision was made for entry into the peritoneal cavity. (B) The Alexis Wound Retractor was inserted through the incision and the wrist portion of a size 7.5 glove was fixed to the outer ring of the wound retractor. (C) External view of the port placement during robotic single-port transumbilical hysterectomy. (D) Post-operative wound on the umbilicus at 4 weeks after surgery.
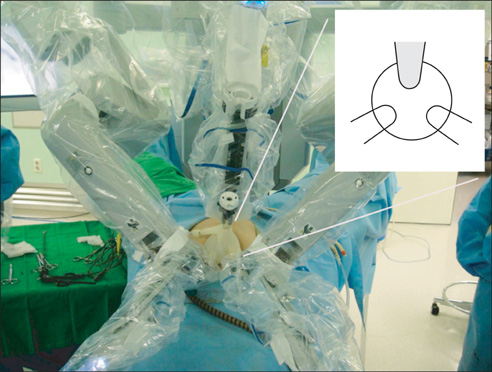
Fig. 2 Robotic single-port transumbilical access system, as seen from the patient's head. The 12-mm port for the robotic 30 degree scope and two 8 mm ports for the robotic instruments were placed in a triangular fashion.
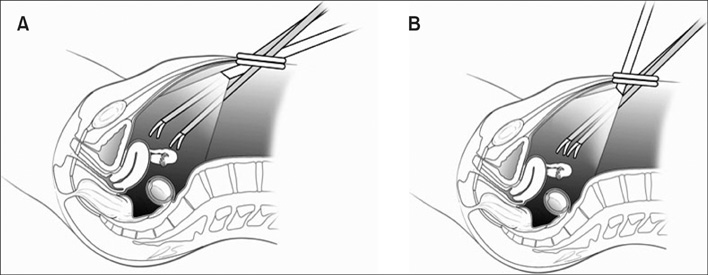
Fig. 3 Position of the robotic camera for robotic single-port transumbilical total hysterectomy to reduce collisions between the instruments and camera. (A) As in the conventional multi-port robotic surgery, if the camera and the instruments are inserted at shallow angles in a 30-degree downward position, collisions between the instruments and camera increase. (B) The 30-degree robotic camera is rotated upward to view the pelvic cavity, which results in fewer collisions between the instruments and camera and provides increased space for instruments to move more freely.
Cited by 1 articles
-
Robotic Single-Site® Sacrocolpopexy: First Report and Technique Using the Single-Site® Wristed Needle Driver
Sa Ra Lee
Yonsei Med J. 2016;57(4):1029-1033. doi: 10.3349/ymj.2016.57.4.1029.
Reference
-
1. Jung YW, Kim YT, Lee DW, Hwang YI, Nam EJ, Kim JH, et al. The feasibility of scarless single-port transumbilical total laparoscopic hysterectomy: initial clinical experience. Surg Endosc. 2010. 24:1686–1692.2. Yim GW, Jung YW, Paek J, Lee SH, Kwon HY, Nam EJ, et al. Transumbilical single-port access versus conventional total laparoscopic hysterectomy: surgical outcomes. Am J Obstet Gynecol. 2010. 203:26e1–e6.3. Escobar PF, Fader AN, Paraiso MF, Kaouk JH, Falcone T. Robotic-assisted laparoendoscopic single-site surgery in gynecology: initial report and technique. J Minim Invasive Gynecol. 2009. 16:589–591.4. Kim TJ, Lee YY, Cha HH, Kim CJ, Choi CH, Lee JW, et al. Single-port-access laparoscopic-assisted vaginal hysterectomy versus conventional laparoscopic-assisted vaginal hysterectomy: a comparison of perioperative outcomes. Surg Endosc. 2010. 24:2248–2252.5. Kim YW, Park BJ, Ro DY, Kim TE. Single-port laparoscopic myomectomy using a new single-port transumbilical morcellation system: initial clinical study. J Minim Invasive Gynecol. 2010. 17:587–592.6. Kim TJ, Lee YY, Kim MJ, Kim CJ, Kang H, Choi CH, et al. Single-port access laparoscopic adnexal surgery. J Minim Invasive Gynecol. 2009. 16:612–615.7. Magrina JF, Zanagnolo VL. Robotic surgery for cervical cancer. Yonsei Med J. 2008. 49:879–885.8. Ramirez PT, Soliman PT, Schmeler KM, dos Reis R, Frumovitz M. Laparoscopic and robotic techniques for radical hysterectomy in patients with early-stage cervical cancer. Gynecol Oncol. 2008. 110:3 Suppl 2. S21–S24.9. Shafer A, Boggess JF. Robotic-assisted endometrial cancer staging and radical hysterectomy with the da Vinci surgical system. Gynecol Oncol. 2008. 111:2 Suppl. S18–S23.10. Kaouk JH, Goel RK, Haber GP, Crouzet S, Stein RJ. Robotic single-port transumbilical surgery in humans: initial report. BJU Int. 2009. 103:366–369.11. Ragupathi M, Ramos-Valadez DI, Pedraza R, Haas EM. Robotic-assisted single-incision laparoscopic partial cecectomy. Int J Med Robot. 2010. 6:362–367.12. Ostrowitz MB, Eschete D, Zemon H, DeNoto G. Robotic-assisted single-incision right colectomy: early experience. Int J Med Robot. 2009. 5:465–470.13. Fader AN, Escobar PF. Laparoendoscopic single-site surgery (LESS) in gynecologic oncology: technique and initial report. Gynecol Oncol. 2009. 114:157–161.14. Magrina JF, Kho RM, Weaver AL, Montero RP, Magtibay PM. Robotic radical hysterectomy: comparison with laparoscopy and laparotomy. Gynecol Oncol. 2008. 109:86–91.15. Quinones GR, Alvarado DA, Ley Ch E. Tubal ligation using Yoon's ring. Ginecol Obstet Mex. 1976. 40:127–136.16. Pelosi MA, Pelosi MA 3rd. Laparoscopic hysterectomy with bilateral salpingo-oophorectomy using a single umbilical puncture. N J Med. 1991. 88:721–726.17. Haber GP, Crouzet S, Kamoi K, Berger A, Aron M, Goel R, et al. Robotic NOTES (Natural Orifice Translumenal Endoscopic Surgery) in reconstructive urology: initial laboratory experience. Urology. 2008. 71:996–1000.18. White MA, Haber GP, Autorino R, Khanna R, Forest S, Yang B, et al. Robotic laparoendoscopic single-site radical prostatectomy: technique and early outcomes. Eur Urol. 2010. 58:544–550.19. Mendivil A, Holloway RW, Boggess JF. Emergence of robotic assisted surgery in gynecologic oncology: American perspective. Gynecol Oncol. 2009. 114:2 Suppl. S24–S31.20. Visco AG, Advincula AP. Robotic gynecologic surgery. Obstet Gynecol. 2008. 112:1369–1384.21. Seamon LG, Backes F, Resnick K, Cohn DE. Robotic trocar site small bowel evisceration after gynecologic cancer surgery. Obstet Gynecol. 2008. 112(2 Pt 2):462–464.22. Sert B. Robotic port-site and pelvic recurrences after robot-assisted laparoscopic radical hysterectomy for a stage IB1 adenocarcinoma of the cervix with negative lymph nodes. Int J Med Robot. 2010. 6:132–135.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single port transumbilical total laparoscopic hysterectomy (TLH): initial experience in Korea
- Transumbilical single port total laparoscopic hysterectomy
- Transumbilical Laparoscopic Cholecystectomy with Additional Port: A Single Surgeon's Experience with 291 Cases
- Single-port plus an additional port robotic complete mesocolic excision and intracorporeal anastomosis using a robotic stapler for right-sided colon cancer
- A comparison of single-port laparoscopically assisted vaginal hysterectomy using transumbilical SILS port access and three-port laparoscopically assisted vaginal hysterectomy
