Microscopic lesions of fallopian tubes in endometrioid carcinoma of the endometrium: How effective are the macroscopic tubal sampling techniques?
- Affiliations
-
- 1Department of Pathology, Hacettepe University Faculty of Medicine, Ankara, Turkey. ausubutu@hacettepe.edu.tr
- KMID: 2288541
- DOI: http://doi.org/10.3802/jgo.2013.24.2.114
Abstract
OBJECTIVE
Extrauterine involvement of endometrial carcinoma has a significant effect on the patients' prognosis and treatment decision. In classical method, macroscopic section is taken from the fallopian tube sparing the fimbrial ends. Fimbrial end of fallopian tube may be involved by tumors and precursor lesions. This study aims to determine the importance of sampling of fimbrial ends of fallopian tube in endometrioid endometrial carcinoma specimens.
METHODS
We reevaluated the fallopian tubes of 200 cases of endometrioid endometrial carcinoma cases that have no macroscopic tubal lesion. A hundred cases were sampled with classical method, and the other 100 were sampled with a new method that includes the fimbrial ends. Statistical difference was examined by Fisher's exact test.
RESULTS
No microscopic tubal lesion lesion was detected in cases that were sampled with the classical method. In contrast, there were 4 cases with tubal lesions in patients sampled with the new technique; 3 of them were located in the fimbrial end. Of the 3, there was one microscopic invasive carcinoma and two proliferative endometrial glandular lesions. Endometriosis was detected in two of the 4 cases with tubal lesions.
CONCLUSION
Including the fimbrial end of fallopian tube to macroscopic sampling could detect more tubal lesions, which might provide additional prognostic and pathogenetic information of endometrioid endometrial carcinoma.
MeSH Terms
Figure
-

Fig. 1 We cut the fallopian tube into two pieces including the fimbrial end (A, B). If the tube measures less than 2 cm, we sample it totally. If it's more than 2 cm, we take a 2 cm sample including the fimbrial end and sample in one cassette (C, D).
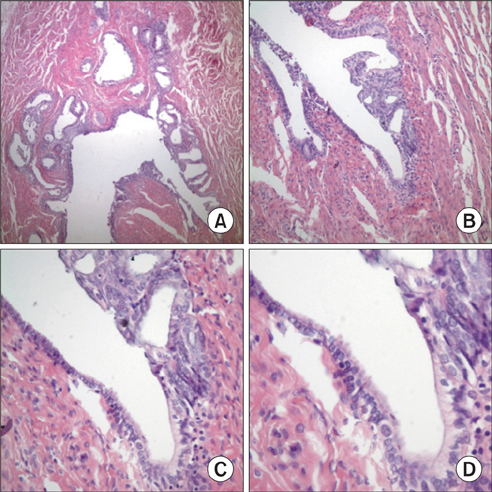
Fig. 2 Presence of endometriosis foci in fallopian tube (A, B). Note the epithelial continuum between tubal epithelium and the endometrioid lesion (C). Closer view of continuum between the lesion and tubal epithelium (D).
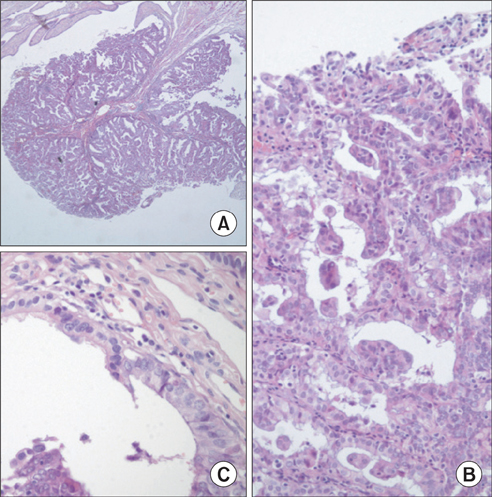
Fig. 3 Focus of infiltrative endometrioid carcinoma; a hanging polypoid lesion in the fimbrial end (A). Closer view of the endometrioid tumor (B). Note the continuity between the carcinoma cells and tubal epithelium (C).

Fig. 4 These proliferative glandular lesions were observed in different areas from the fallopian tubes of the same patient (A-C) and continuum between normal tubal epithelium and the proliferative lesion can easily be seen in both lesions (C, D).
Cited by 1 articles
-
Comparison of the Classical Method and SEE-FIM Protocol in Detecting Microscopic Lesions in Fallopian Tubes with Gynecological Lesions
Nermin Koc, Selçuk Ayas, Sevcan Arzu Arinkan
J Pathol Transl Med. 2018;52(1):21-27. doi: 10.4132/jptm.2016.06.17.
Reference
-
1. Wright JD, Barrena Medel NI, Sehouli J, Fujiwara K, Herzog TJ. Contemporary management of endometrial cancer. Lancet. 2012. 379:1352–1360.2. Medeiros F, Muto MG, Lee Y, Elvin JA, Callahan MJ, Feltmate C, et al. The tubal fimbria is a preferred site for early adenocarcinoma in women with familial ovarian cancer syndrome. Am J Surg Pathol. 2006. 30:230–236.3. Przybycin CG, Kurman RJ, Ronnett BM, Shih IeM, Vang R. Are all pelvic (nonuterine) serous carcinomas of tubal origin? Am J Surg Pathol. 2010. 34:1407–1416.4. Roh MH, Kindelberger D, Crum CP. Serous tubal intraepithelial carcinoma and the dominant ovarian mass: clues to serous tumor origin? Am J Surg Pathol. 2009. 33:376–383.5. Vigano P, Somigliana E, Chiodo I, Abbiati A, Vercellini P. Molecular mechanisms and biological plausibility underlying the malignant transformation of endometriosis: a critical analysis. Hum Reprod Update. 2006. 12:77–89.6. Culton LK, Deavers MT, Silva EG, Liu J, Malpica A. Endometrioid carcinoma simultaneously involving the uterus and the fallopian tube: a clinicopathologic study of 13 cases. Am J Surg Pathol. 2006. 30:844–849.7. Himmetoglu C, Usubutun A, Ayhan A, Kucukali T. Incidental serous papillary ovarian carcinoma diagnosed on endometrial biopsy. Turk J Pathol. 2008. 24:186–189.8. Usubutun A. Hilus cells in tuba uterina; an uncommon localisation and coincidence with endometrial carcinoma: a case report and review of the literature. Turk J Pathol. 2007. 23:52–55.9. Auersperg N. The origin of ovarian carcinomas: a unifying hypothesis. Int J Gynecol Pathol. 2011. 30:12–21.10. Kuhn E, Kurman RJ, Vang R, Sehdev AS, Han G, Soslow R, et al. TP53 mutations in serous tubal intraepithelial carcinoma and concurrent pelvic high-grade serous carcinoma--evidence supporting the clonal relationship of the two lesions. J Pathol. 2012. 226:421–426.11. Kurman RJ, Shih IeM. The origin and pathogenesis of epithelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol. 2010. 34:433–443.12. Kurman RJ, Vang R, Junge J, Hannibal CG, Kjaer SK, Shih IeM. Papillary tubal hyperplasia: the putative precursor of ovarian atypical proliferative (borderline) serous tumors, noninvasive implants, and endosalpingiosis. Am J Surg Pathol. 2011. 35:1605–1614.13. Navani SS, Alvarado-Cabrero I, Young RH, Scully RE. Endometrioid carcinoma of the fallopian tube: a clinicopathologic analysis of 26 cases. Gynecol Oncol. 1996. 63:371–378.14. Alvarado-Cabrero I, Navani SS, Young RH, Scully RE. Tumors of the fimbriated end of the fallopian tube: a clinicopathologic analysis of 20 cases, including nine carcinomas. Int J Gynecol Pathol. 1997. 16:189–196.15. Axelrod JH, Fruchter R, Boyce JG. Multiple primaries among gynecologic malignancies. Gynecol Oncol. 1984. 18:359–372.16. Eisner RF, Nieberg RK, Berek JS. Synchronous primary neoplasms of the female reproductive tract. Gynecol Oncol. 1989. 33:335–339.17. Clement PB. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv Anat Pathol. 2007. 14:241–260.18. Rosai J. Surgical pathology. 2011. 10th ed. St. Louis, MO: Mosby Elsevier.19. Kurman RJ, editor. Blaustein's pathology of the female genital tract. 2002. 5th ed. New York: Springer-Verlag.20. Kurman RJ, Ellenson LH, Ronnett BM, editors. Blaustein's pathology of the female genital tract. 2011. 6th ed. New York: Springer-Verlag.21. Dietl J, Wischhusen J, Hausler SF. The post-reproductive Fallopian tube: better removed? Hum Reprod. 2011. 26:2918–2924.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of the Classical Method and SEE-FIM Protocol in Detecting Microscopic Lesions in Fallopian Tubes with Gynecological Lesions
- Synchronous Papillary Tumor of the Fallopian Tube and Endometrium: A Case Report
- Benign Teratomas of the Fallopian Tubes: A report of two cases
- An Unsuspected Primary Tubal Carcinoma During Operative Laparoscopy
- Isolated Torsion of Fallopian Tubes: Detection of Pedicle at Tubal End: Two Case Report
