Breast Metastasis from Rhabdomyosarcoma of the Anus in an Adolescent Female
- Affiliations
-
- 1Division of Breast and Endocrine Surgery, Department of Surgery, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
- 2Department of Pediatrics, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Breast and Endocrine Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jeongeon.lee@samsung.com
- 5Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2286388
- DOI: http://doi.org/10.4048/jbc.2013.16.3.345
Abstract
- Rhabdomyosarcoma (RMS) of the breast is rare and there is scant information about the clinical behavior and treatment strategies. We report an adolescent female patient with metastatic RMS of the breast from the anus. An 18-year-old female patient was referred to our clinic due to palpable mass in the left breast. At age seven, she was diagnosed with acute lymphoblastic leukemia and treated with chemoradiation therapy. After 10 years of complete remission state, she presented with anal mass which was diagnosed as RMS and she received chemoradiation therapy. After 1 year of complete remission state, she noticed a palpable mass in her left breast. The breast mass was diagnosed as metastatic RMS based on core needle biopsy specimen. The RMS in breast was excised for the decreasing tumor burden despite of another metastatic lesion. Although rarely reported, metastasis of RMS should be considered as a cause of breast mass. Tissue biopsy is recommended when clinically suspected lesion is detected.
Keyword
MeSH Terms
Figure
-
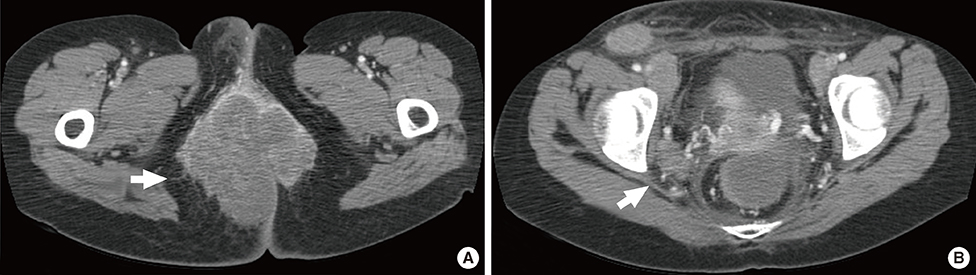
Figure 1 Computed tomography image of anal rhabdomyosarcoma. (A) Heterogenous enhancing mass, 8.5 cm sized in largest diameter, was noted around anus on computed tomography. (B) About 2.5 cm sized, enlarged lymph nodes were located around right iliac vessel (white arrow) and both inguinal area suggesting multiple lymph nodes metastasis.

Figure 2 Image of metastatic rhabdomyosarcoma. (A) A 2.3 cm sized round and circumscribed mass was found on breast ultrasonography. Positron emission tomography/computed tomography scan demonstrates hot uptake on left upper outer breast (B) and right retrocrural area (C).
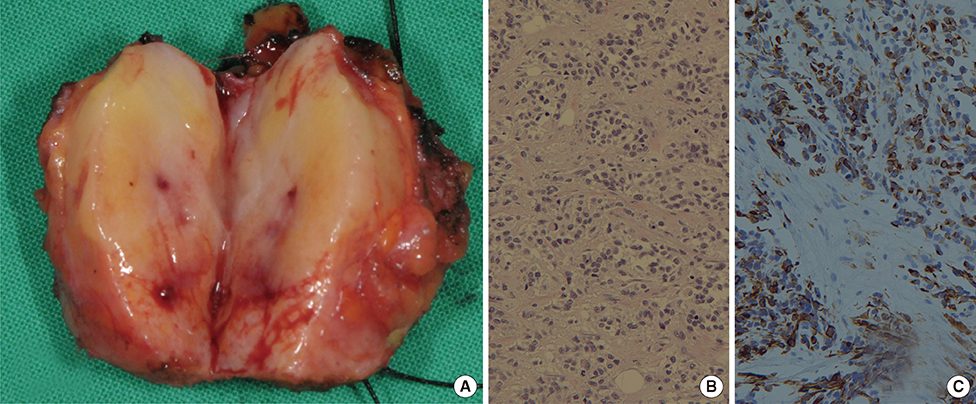
Figure 3 Histologic findings of metastatic rhabdomyosarcoma in breast. (A) The rhabdomyosarcoma was oval and well-circumscribed, 2.2 cm sized in diameter. The cut surface showed focal hemorrhage with white central compartment encircled by yellow area. The small round cells are arranged in variably sized nest by fibrous tissue septa (H&E stain, ×200) (B) and strongly stained with desmin immunohistochemical stain (desmin stain, ×200) (C).
Reference
-
1. Binokay F, Soyupak SK, Inal M, Celiktas M, Akgül E, Aksungur E. Primary and metastatic rhabdomyosarcoma in the breast: report of two pediatric cases. Eur J Radiol. 2003; 48:282–284.
Article2. Pollard SG, Marks PV, Temple LN, Thompson HH. Breast sarcoma: a clinicopathologic review of 25 cases. Cancer. 1990; 66:941–944.
Article3. D'Angelo P, Carli M, Ferrari A, Manzitti C, Mura R, Miglionico L, et al. Breast metastases in children and adolescents with rhabdomyosarcoma: experience of the Italian Soft Tissue Sarcoma Committee. Pediatr Blood Cancer. 2010; 55:1306–1309.4. Italiano A, Largillier R, Peyrottes I, Hannoun-Levy JM, Lallement M, Thyss A. Primary embryonal rhabdomyosarcoma of the breast in an adult female. Breast J. 2005; 11:214.
Article5. Gaynon PS, Steinherz PG, Bleyer WA, Ablin AR, Albo VC, Finklestein JZ, et al. Improved therapy for children with acute lymphoblastic leukemia and unfavorable presenting features: a follow-up report of the Childrens Cancer Group Study CCG-106. J Clin Oncol. 1993; 11:2234–2242.
Article6. Hays DM, Donaldson SS, Shimada H, Crist WM, Newton WA Jr, Andrassy RJ, et al. Primary and metastatic rhabdomyosarcoma in the breast: neoplasms of adolescent females, a report from the Intergroup Rhabdomyosarcoma Study. Med Pediatr Oncol. 1997; 29:181–189.
Article7. Howarth CB, Caces JN, Pratt CB. Breast metastases in children with rhabdomyosarcoma. Cancer. 1980; 46:2520–2524.
Article8. Li DL, Zhou RJ, Yang WT, Wang J, Yao XH, Cheng YF, et al. Rhabdomyosarcoma of the breast: a clinicopathologic study and review of the literature. Chin Med J. 2012; 125:2618–2622.9. Ahn SJ, Kim SK, Kim EK. Metastatic breast cancer from rhabdomyosarcoma mimicking normal breast parenchyma on sonography. J Ultrasound Med. 2010; 29:489–492.
Article10. Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ. WHO Classification of Tumours of the Breast. 4th ed. Lyon: International Agency for Research on Cancer;2012. p. 48–146.11. Schmiegelow K, Levinsen MF, Attarbaschi A, Baruchel A, Devidas M, Escherich G, et al. Second malignant neoplasms after treatment of childhood acute lymphoblastic leukemia. J Clin Oncol. 2013; 31:2469–2476.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Unusual Imaging Finding of Breast Metastasis from Rhabdomyosarcoma
- A Case of Paratesticular Rhabdomyosarcoma
- Metastasis of Rhabdomyosarcoma to the Male Breast: a Case Report with Magnetic Resonance Imaging Findings
- A Case of Orbital Rhabdomyosarcoma
- Four Cases of Rhabdomyosarcoma in the Head and Neck
