Intest Res.
2014 Apr;12(2):162-165. 10.5217/ir.2014.12.2.162.
A Case of Ascending Colonic Xanthoma Presenting as a Lateral Spreading Tumor
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. dshskim@jnu.ac.kr
- 2Department of Pathology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2284903
- DOI: http://doi.org/10.5217/ir.2014.12.2.162
Abstract
- Gastrointestinal xanthomas are characterized by foamy cytoplasmic cells containing lipid in lamina propria, and occur almost in the gastric mucosa. Colonic xanthomas have been described in rare case. All reported colonic xanthomas were located in rectosigmoid. Rectosigmoid xanthomas have tended to exhibit small polypoid lesion, on the contrary flat in stomach. We report a case of xanthoma on ascending colon presenting as a laterally spreading tumor resected by endoscopic mucosal resection method.
Keyword
Figure
-
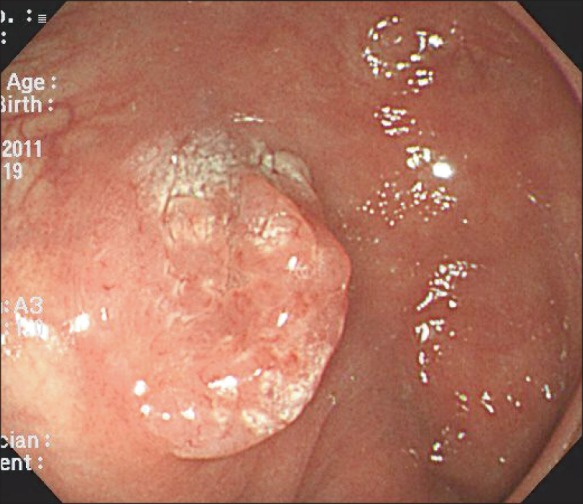
Fig. 1 Colonoscopic findings. The endoscopy showed about 15 mm sized laterally spreading tumor in the ascending colon.
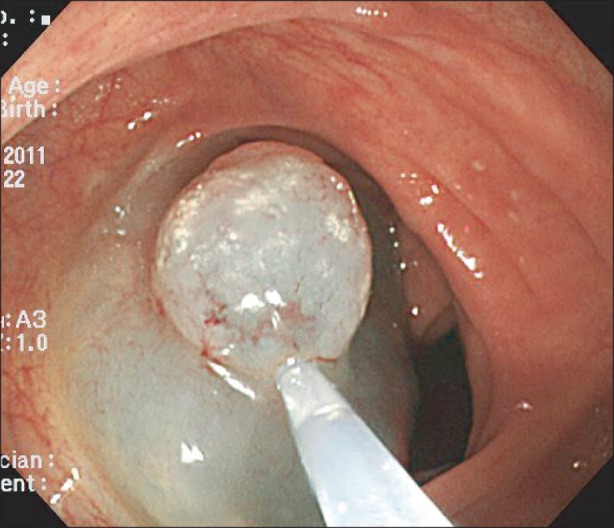
Fig. 2 Endoscopic treatment. Endoscopic mucosal resection using saline injection and snare was conducted.

Fig. 3 Histopathological finding. Multiple foamy cells are noted in lamina propria (H&E stain, ×100).
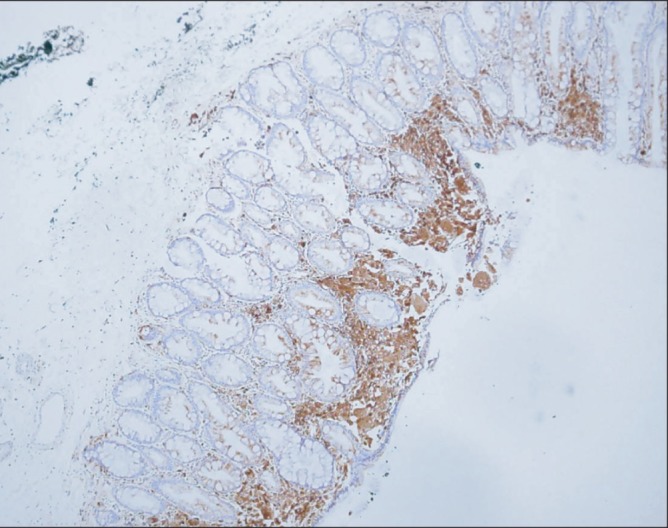
Fig. 4 Immunohistochemical stain (IHCS) finding. Foamy cells are positive for CD68 IHCS (×100).
Reference
-
1. Nakasono M, Hirokawa M, Muguruma N, et al. Colorectal xanthomas with polypoid lesion: report of 25 cases. APMIS. 2004; 112:3–10. PMID: 14961968.
Article2. Kim CH, Cho JY, Lim SB, et al. A case of gastric xanthomatosis scattered through whole gastric mucosa. Korean J Gastrointest Endosc. 1990; 10:317–320.3. Gencosmanoglu R, Sen-Oran E, Kurtkaya-Yapicier O, Tozun N. Xanthelasmas of the upper gastrointestinal tract. J Gastroenterol. 2004; 39:215–219. PMID: 15064997.
Article4. Khachaturian T, Dinning JP, Earnest DL. Gastric xanthelasma in a patient after partial gastrectomy. Am J Gastroenterol. 1998; 93:1588–1589. PMID: 9732956.
Article5. Remmele W, Beck K, Kaiserling E. Multiple lipid islands of the colonic mucosa. A light and electron microscopic study. Pathol Res Pract. 1988; 183:336–346. PMID: 3420034.
Article6. Miliauskas JR. Rectosigmoid (colonic) xanthoma: a report of four cases and review of the literature. Pathology. 2002; 34:144–147. PMID: 12009096.
Article7. Bejarano PA, Aranda-Michel J, Fenoglio-Preiser C. Histochemical and immunohistochemical characterization of foamy histiocytes (muciphages and xanthelasma) of the rectum. Am J Surg Pathol. 2000; 24:1009–1015. PMID: 10895824.
Article8. Coates AG, Nostrant TT, Wilson JA, Dobbins WO 3rd, Agha FP. Gastric xanthomatosis and cholestasis. A causal relationship. Dig Dis Sci. 1986; 31:925–928. PMID: 3731984.9. Isomoto H, Mizuta Y, Inoue K, et al. A close relationship between Helicobacter pylori infection and gastric xanthoma. Scand J Gastroenterol. 1999; 34:346–352. PMID: 10365893.
Article10. Moran AM, Fogt F. 70-year-old female presenting with rectosigmoid (colonic) xanthoma and multiple benign polyps - case report. Pol J Pathol. 2010; 61:42–45. PMID: 20496273.11. Boruchowicz A, Rey C, Fontaine M, et al. Colonic xanthelasma due to glyceride accumulation associated with an adenoma. Am J Gastroenterol. 1997; 92:159–161. PMID: 8995960.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Ascending Colonic Diverticulum Presenting With Intussusception
- Submerging Endoscopic Submucosal Dissection Leads to Successful En Bloc Resection of Colonic Laterally Spreading Tumor with Submucosal Fat
- A Case of Type IV Hyperlipoproteinemia with Palmar Xanthoma, Tuberous Xanthoma, and Eruptive Xanthoma
- A Case of B-Lymphoblastic Leukemia/Lymphoma Detected as a Laterally Spreading Tumor
- Bladder Xanthoma
