Disseminated Tuberculosis in a Patient with Chronic Renal Failure
- Affiliations
-
- 1Department of Internal Medicine, Ewha Womans University School of Medicine, Seoul, Korea. drryu@ewha.ac.kr
- KMID: 2284018
- DOI: http://doi.org/10.12771/emj.2013.36.1.67
Abstract
- Patients with chronic renal failure (CRF) are known to be more susceptible to tuberculosis infection due to impairment of the host defense mechanism. Although extrapulmonary tuberculosis is more prevalent in those subjects and it may induce dismal outcome, its diagnosis has been challenging since there is no specific symptoms of the disease and the clinical course is usually atypical. Herein, We report a case of disseminated tuberculosis diagnosed by ultrasound-guided liver biopsy in a 31-year-old CRF patient presenting sustained fever despite broad-spectrum antimicrobial therapy and progressive cholestatic jaundice.
Figure
-
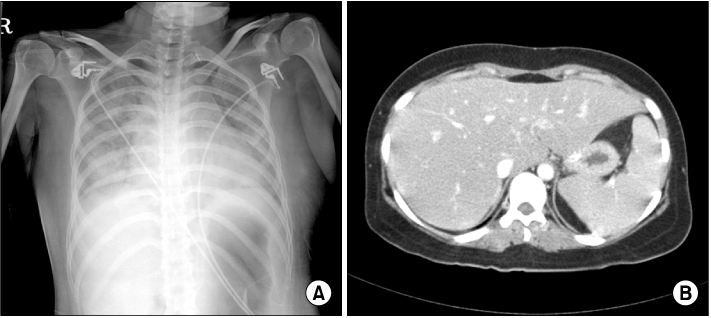
Fig. 1 Initial radiologic findings. Chest X-ray shows pulmonary edema and cardiomegaly, while there is no evidence of pulmonary or miliary tuberculosis (A). Hepatomegaly and splenomegaly without abnormal enhancement in the liver is noted in abdominal computed tomography (B).
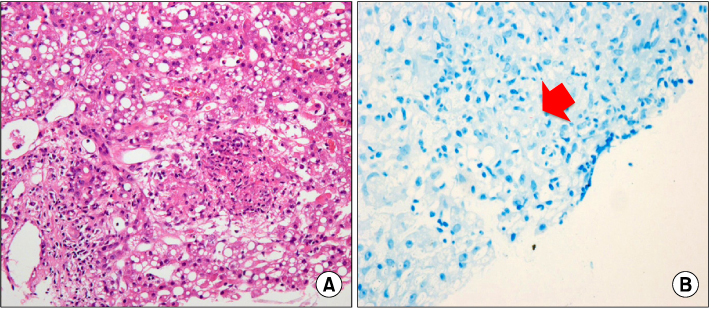
Fig. 2 Histopathologic findings of the liver. There are scattered non-caseating granulomas with focus of multinucleated giant cell (A: H&E, ×200). The acid-fast bacilli are stained (B), and arrow indicates the bacilli (Ziehl-Neelsen stain, ×400).
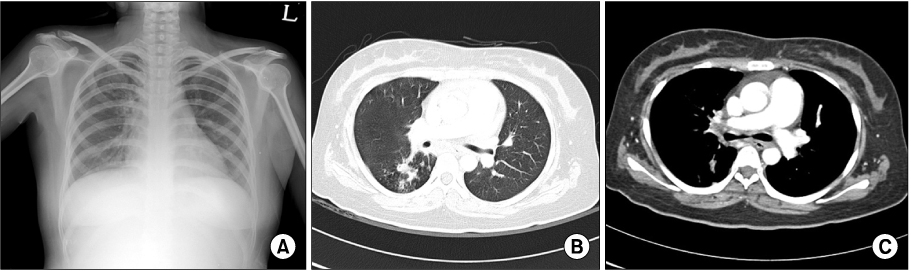
Fig. 3 Chest radiographic images for the evaluation of orthopnea performed after 25 days of the start of anti-tuberculosis medication. Chest posterioranterior X-ray shows that focal consolidations are seen in right upper lung field (A). Active pulmonary tuberculosis is seen in right upper lobe (B), and right and left main bronchus is narrowing with enhanced wall thickening (C) in the chest computed tomography.
Reference
-
1. World Health Organization. Global tuberculosis control report 2012. 2012. Geneva: World Health Organization.2. Korea Center for Disease Control and Prevention. Korean Institute of Tuberculosis. Annual report on the notified tuberculosis patients in Korea. 2011. Seoul: Korean Institute of Tuberculosis.3. Hussein MM, Mooij JM, Roujouleh H. Tuberculosis and chronicrenal disease. Semin Dial. 2003. 16:38–44.4. Choi BK, Lee HS, Hwang IH, Shin KH, Choi MK, Choi BG, et al. Comparative analysis of the clinical features and prognosis of extrapulmonary tuberculosis according to the renal function. Korean J Med. 2010. 79:387–393.5. Yoon SY, Choi SR, Kang EW, Goo YS, Kim BS, Youn HJ, et al. Clinical features of tuberculosis in dialysis patients. Korean J Nephrol. 2003. 22:73–79.6. ESRD Registry Committee, Korean Society of Nephrology. Current renal replacement therapy in Korea-Insan memorial dialysis registry 2008. Korean J Nephrol. 2009. 28:S498–S510.7. Korea National Statistical Office. Deaths and death rate by cause. 2008. Daejeon: Korea National Statistical Office.8. Chia S, Karim M, Elwood RK, FitzGerald JM. Risk of tuberculosis in dialysis patients: a population based study. Int J Tuberc Lung Dis. 1998. 2:989–991.9. Descamps-Latscha B, Herbelin A, Nguyen AT, Jungers P, Chatenoud L. Dysregulation of the immune system in chronic uremicand hemodialysed patients. Presse Med. 1995. 24:405–410.10. Vanholder R, Ringoir S. Polymorphonuclear cell function and infection in dialysis. Kidney Int Suppl. 1992. 38:S91–S95.11. Powe NR, Jaar B, Furth SL, Hermann J, Briggs W. Septicemia in dialysis patients: incidence, risk factors, and prognosis. Kidney Int. 1999. 55:1081–1090.12. Moon GH, Song JH, Lee SW, Lee KJ, Park HS, Kim MJ. Hepatic tuberculous abscess and miliary tuberculosis in a gemodialysis patient. Korean J Nephrol. 2001. 20:332–336.13. US Department of Health and Human Services. Reported tuberculosis in the United States. 2002. Atlanta, GA: Centers for Disease Control and Prevention.14. Klatskin G. Schiff L, editor. Hepatitis associated with systemic infections. Disease of the liver. 1975. Philadelphia: J. B. Lippincott;711.15. Godwin JE, Coleman AA, Sahn SA. Miliary tuberculosis presenting as hepatic and renal failure. Chest. 1991. 99:752–754.16. Hussain W, Mutimer D, Harrison R, Hubscher S, Neuberger J. Fulminant hepatic failure caused by tuberculosis. Gut. 1995. 36:792–794.17. Sharma SK, Shamim SQ, Bannerjee CK, Sharma BK. Disseminated tuberculosis presenting as massive hepatosplenomegaly and hepatic failure. Case report. Am J Gastroenterol. 1981. 76:153–156.18. Essop AR, Posen JA, Hodkinson JH, Segal I. Tuberculosis hepatitis: a clinical review of 96 cases. Q J Med. 1984. 53:465–477.19. Kang GH, Kim YI, Kim CW. Confirmation of tuberculosis hepatitis using polymerase chain reaction. Korean J Gastroenterol. 1997. 30:415–419.20. Wilfredo T, Rodolfo M, Klaus-Dieter K, Ari K. Friedman LN, editor. Extrapulmonary tuberculosis. Tuberculosis, current concepts and treatment. 2001. 2nd ed. Boca Raton: CRC Press;139–190.21. Wang JY, Hsueh PR, Wang SK, Jan IS, Lee LN, Liaw YS, et al. Disseminated tuberculosis: a 10-year experience in a medical center. Medicine (Baltimore). 2007. 86:39–46.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Disseminated Bone Tuberculosis
- Clinical menifestations of tuberculosis in chronic renal failure
- Clinical Experience of Hemodialysis on Three Cases of Renal Failure using Kill Type Artificial Kidney
- Two cases of disseminated tuberculosis associated with the myelodysplastic syndrome
- Successful Treatment of Neonatal Herpes Simplex Infection Presenting as Fulminant Hepatitis with Acyclovir and Peritoneal Dialysis
