The Size of the Rotator Cuff and the Positional Relationship of Bony Landmarks: An Anatomical Study
- Affiliations
-
- 1Department of Anatomy, College of Medicine, The Catholic University of Korea. ibkimmd@catholic.ac.kr
- 2Catholic Institute for Applied Anatomy, College of Medicine, The Catholic University of Korea.
- 3Department of Anatomy, College of Medicine, The Chung-Ang University of Korea.
- KMID: 2283742
- DOI: http://doi.org/10.11637/kjpa.2015.28.1.11
Abstract
- For treatment of the rotator cuff, locating the structure and position of the rotator cuff is crucial. The aim of this study is to identify the size of each rotator cuff and the locational relationship with bony landmarks, and to provide superficial landmarks for locating the tendon from the surface. Fifty-two shoulders from 26 cadavers were dissected and measured in a supine position. The central point was set as the most protrusive point on the greater tubercle of the humerus. The measurement of angles was described ventral as positive (+) and dorsal as negative (-) placing the long axis of the humeral shaft at 0degrees. The range of the angle which each rotator cuff tendon is attached to the humerus head was: 53.8~103.3 degrees for the subscapularis, -17.1~25.7 degrees for the supraspinatus, -68.4~-1.9 degrees for the infraspinatus, and -117.1~-75.7 degrees for the teres minor. The vertical inferior point drawn from the anterior edge of the acromion to the humerus was 7.5+/-11.7 degrees from the central point. The average position of the point was the midpoint of insertion of the supraspinatus tendon. The lateral horizontal point drawn from the acromial angle to the humerus was -49.4+/-14.3 degrees away and located at an average of 30% inferior to the infraspinatus tendon. Also the lateral horizontal point drawn from the most protrusive point of the coracoid process to the humerus was 63.1+/-14.7 degrees away and located at an average of 20% superior to the subscapularis tendon. Lastly, the most protrusive point of the lesser tubercle of the humerus was located at a range of 80.8+/-11.1 degrees and an average of 60% superior to the insertion of the subscapularis tendon. For the measurements of the size of the rotator cuff, there was no statistical difference between the left and right. However, the four measurements - the proximal width of the teres minor tendon, the proximal and distal width, and the length of the subscapularis tendon - showed statistically significant difference between the sexes (P<0.05). Therefore, to identify the location of the tendon structures by palpation for shoulder treatment, using the lesser tubercle for the subscapularis, the anterior edge of the acromion for the supraspinatus, and the acromial angle for the infraspinatus as landmarks is regarded to be effective.
MeSH Terms
Figure
-
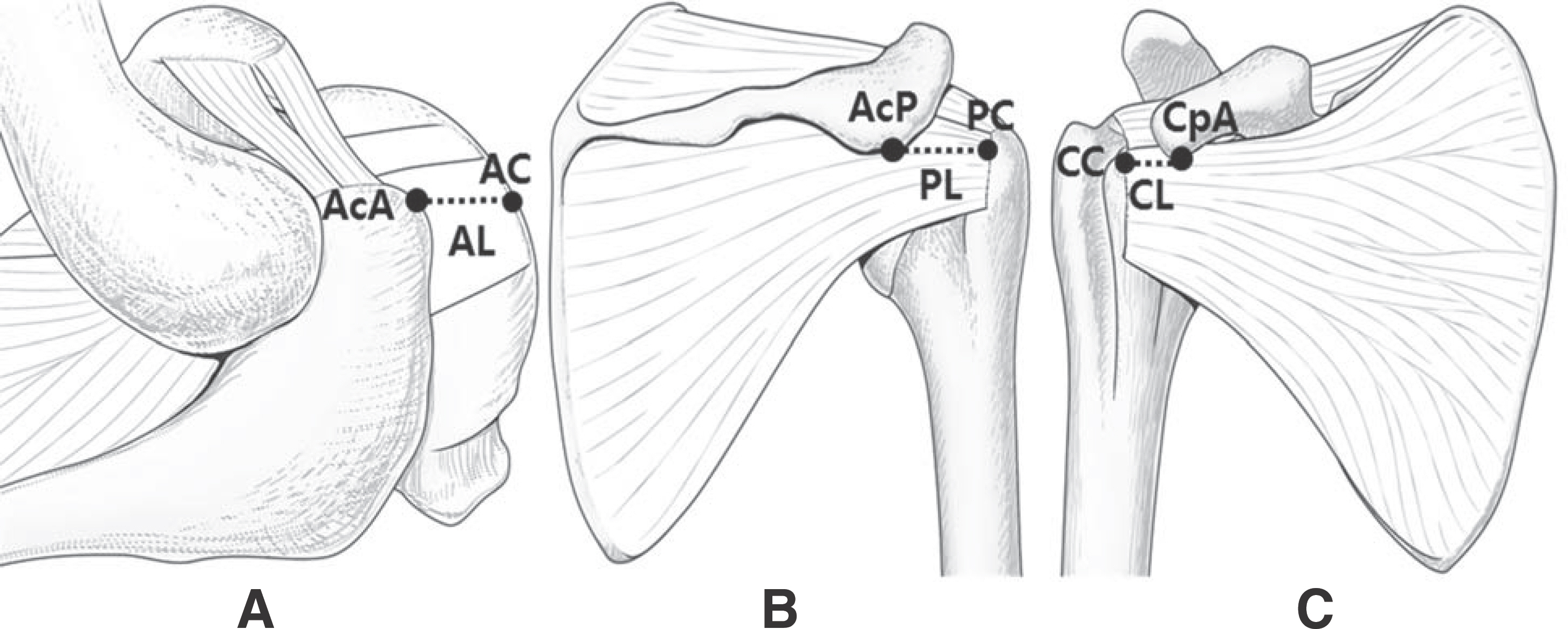
Fig. 1a. The distance between the proximal end of tendon and the bony landmarks. (A) Superior view of the shoulder joint. (B) Posterior view of the shoulder joint. (C) Anterior view of the shoulder joint. AcA, Anterior edge of acromion; AC, A point vertically drawn down from the AcA; AL, The distance from AcA to AC; AcP, Posterior edge of acromion; PC, A point lateral-horizontally drawn from the AcP; PL, The distance from AcP to PC; CpA, Anterior edge of coracoid process; CC, A point lateral-horizontally drawn from the most protrusive point of the CpA; CL, The distance from CpA to CC.
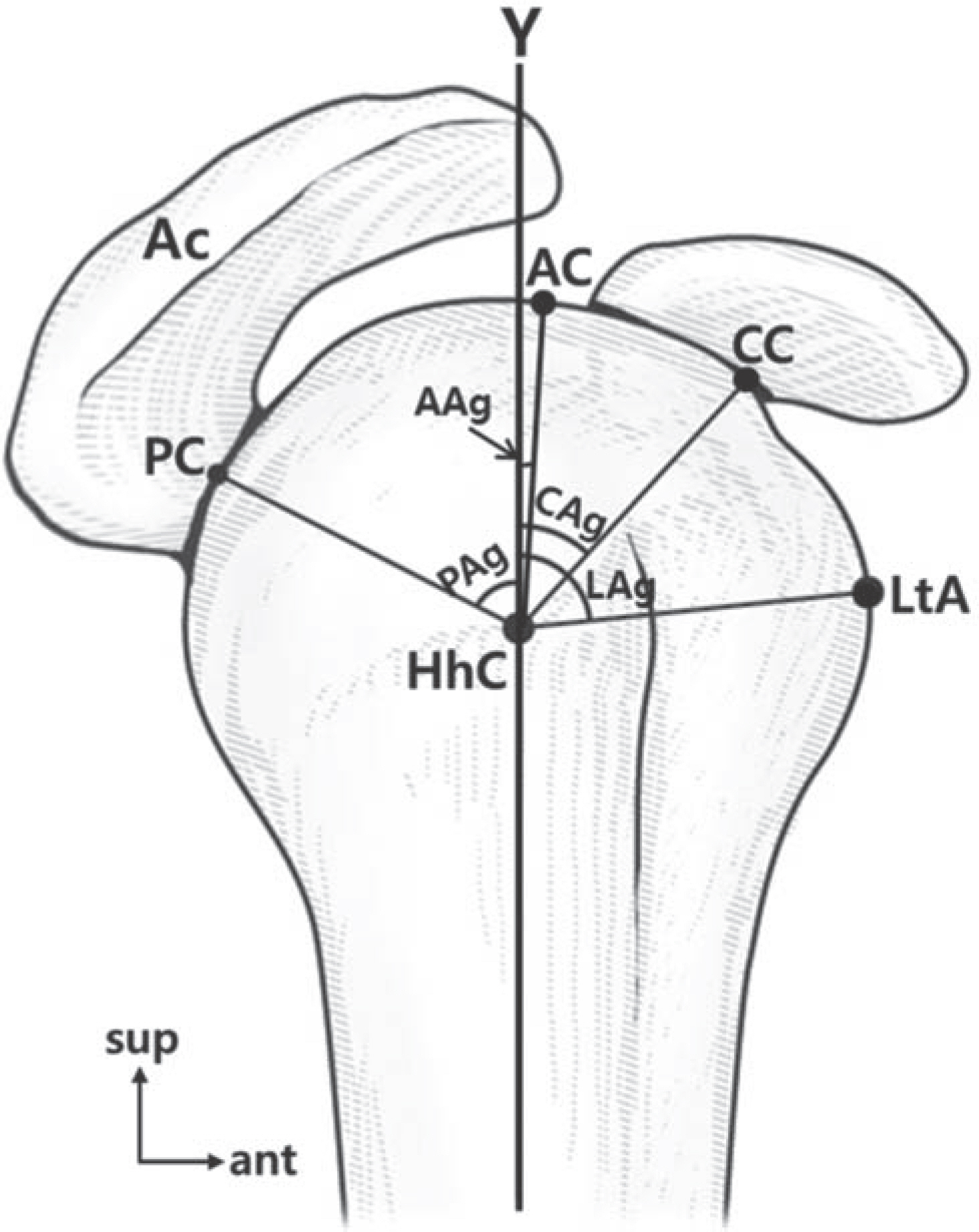
Fig. 1b. The locational relationship between the rotator cuff and the bony landmarks. Ac, Acromion; HhC, Central point of humeral head; LtA, Anterior edge of lesser tubercle; PAg, Angle of PC-HhC-Y; AAg, Angle of AC-HhC-Y; CAg, Angle of CC-HhC-Y; LAg, Angle of LtA-HhC-Y.
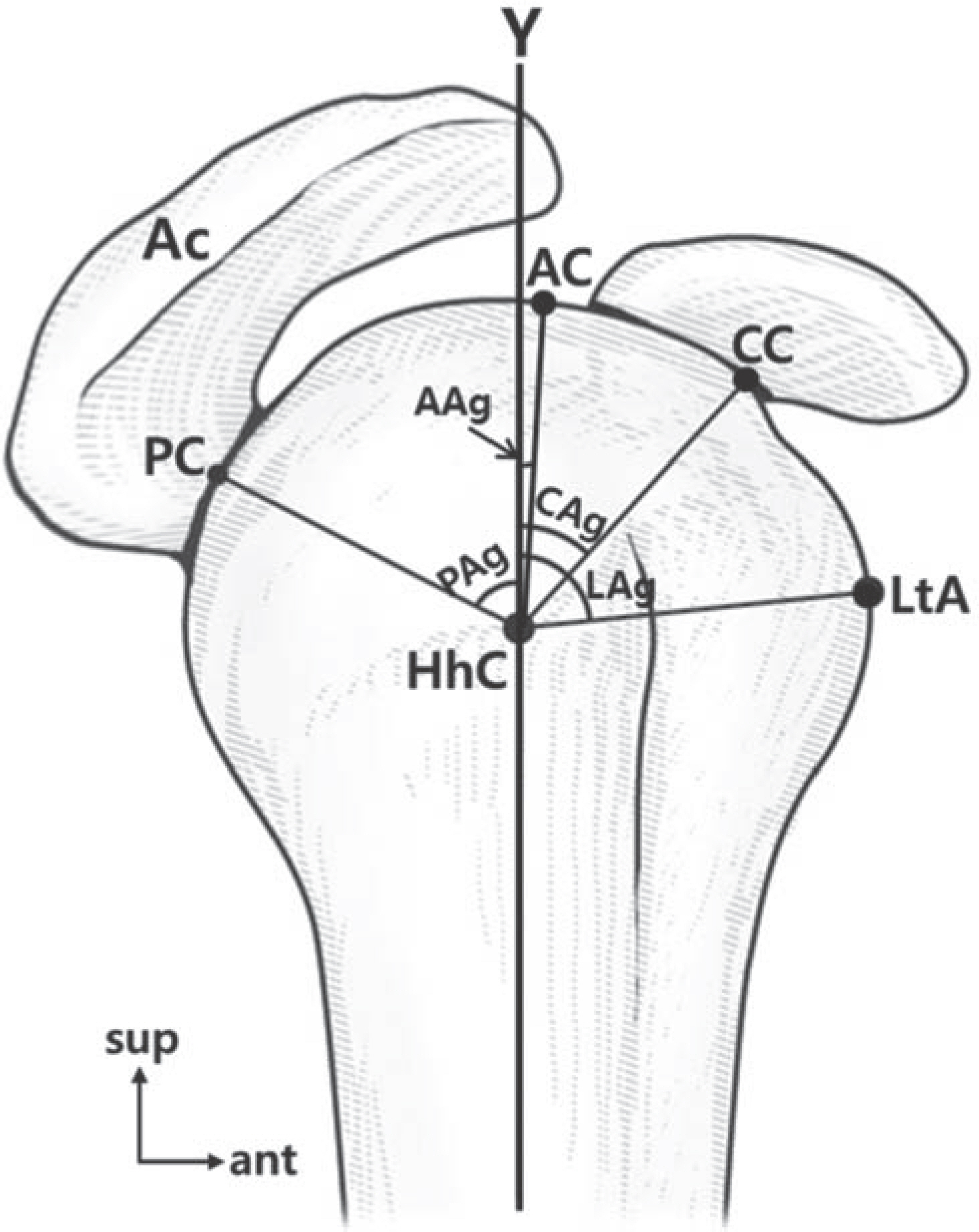
Fig. 2. The range of angles that the rotator cuff tendon attaches to the humerus with respect to the central point. Gray color, The ro-tator cuff tendons; Dark gray color, Overlapping region of the sup-raspinatus tendon and the infraspinatus tendon; SS, tendon of Sub-scapularis; ISP, tendon of Infraspinatus; SSP, tendon of Supraspi-natus; TM, tendon of Teres minor; HhC, central point.
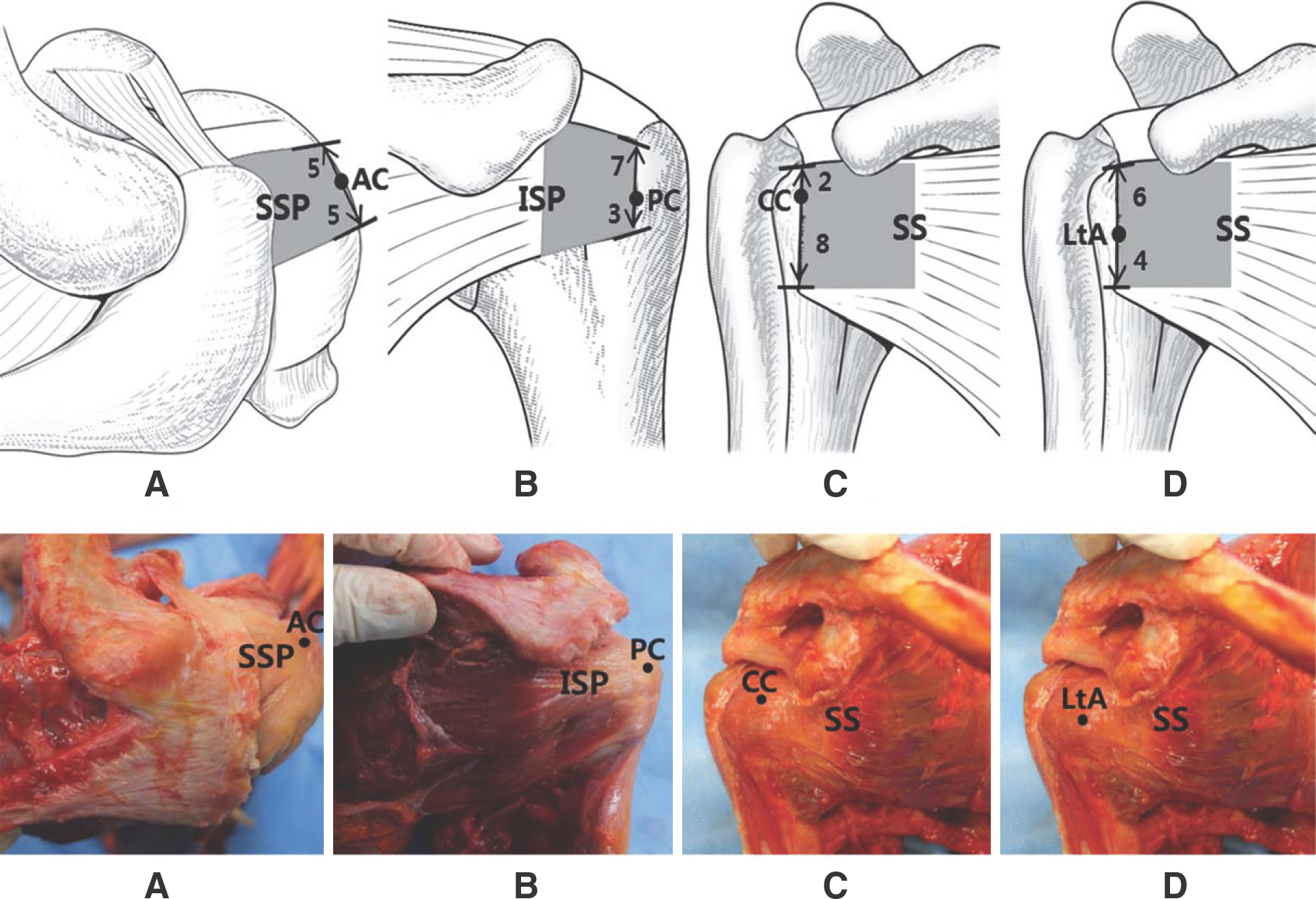
Fig. 3. The locational relationship between the rotator cuff and bony landmarks. (A) Location of the AC on the SSP. (B) Location of the PC on the ISP. (C) Location of the CC on the SS. (D) Location of the LtA on the SS. SSP, Supraspinatus; AC, A point vertically drawn down from the AcA; ISP, Infraspinatus; PC, A point lateral-horizontally drawn from the AcP; SS, Subscapularis; CC, A point lateral-horizontally drawn from the most protrusive point of the CpA; LtA, The most protrusive point of the LtA; Gray color, The rotator cuff tendons.
Reference
-
References
1. DePalma AF. The classic. Surgical anatomy of the rotator cuff and the natural history of degenerative periarthritis. Clin Orthop Relat Res. 2008; 466:543–51.2. Lhee SH, Kho DH, Park JY. Shoulder Operation. J Korean Med Assoc. 2009; 52:795–804.
Article3. De Beer J. Corticosteriod Injections in the shoulder. Pain Med. 2011; 12:1449.
Article4. Kirchhoff C, Kirchhoff S, Sprecher CM, Ahrens P, Imhoff AB, Hinterwimmer S, et al. X-treme CT analysis of cancellous bone at the rotator cuff insertion in human individuals with osteoporosis: superficial versus deep quality. Arch Orthop trauma Surg. 2013; 133:381–87.
Article5. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev. 2003. CD004016.
Article6. Mochizuki T, Sugaya H, Uomizu M, Maeda K, Matsuki K, Sekiya I, et al. Humeral insertion of the supraspinatus and infraspinatus. New anatomical findings regarding the footprint of the rotator cuff. J Bone Joint Surg Am. 2009; 91:1–7.
Article7. Longo UG, Franceschi F, Berton A, Maffulli N, Denaro V. Arthroscopic transosserous rotator cuff repair. Med sport Sci. 2012; 57:142–52.8. Saunders S, Longworth S, Maddison P. Injection techniques in orthopaedic and sports medicine. 2nd ed.West Washington: W. B. Saunders;2002.9. Park JY, Siti HT, O KS, Chung KT, Lee JY, Oh JH. Blind subacromial injection from the anterolateral approach: the ballooning sign. J Shoulder Elbow Surg. 2010; 19:1070–5.
Article10. Minagawa H, Itoi E, Konno N, Kido T, Sano A, Urayama M, et al. Humeral attachment of the supraspinatus and infra-spinatus tendons: an anatomic study. Arthroscopy. 1998; 14:302–6.
Article11. Curtis AS, Burbank KM, Tierney JJ, Scheller AD, Curran AR. The insertional footprint of the rotator cuff: an anatomic study. Arthroscopy. 2006; 22:603–9.
Article12. Goupille P, Sibilia J. Local corticosteroid injections in the treatment of rotator cuff tendinitis. Clin Exp Dermatol. 1996; 14:561–66.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Bony Procedure During of Rotator Cuff Repair: Acromioplasty, Distal Clavicle Resection, Footprint Preparation and Coracoplasty
- Biological Characteristics of Rotator Cuff Tendon
- Patch Augmentation for Massive Rotator Cuff Tears
- Relationship of Posterior Decentering of the Humeral Head with Tear Size and Fatty Degeneration in Rotator Cuff Tear
- Revisional Rotator Cuff Repair
