Diabetes Metab J.
2013 Apr;37(2):132-139. 10.4093/dmj.2013.37.2.132.
Low Levels of Physical Activity Are Associated with Increased Metabolic Syndrome Risk Factors in Korean Adults
- Affiliations
-
- 1Department of Sport and Leisure Studies, Yonsei University College of Sciences in Education, Seoul, Korea. jjeon@yonsei.ac.kr
- 2University College, Yonsei International Campus, Incheon, Korea.
- 3Department of Exercise and Sports Science, Jeju National University College of Natural Sciences, Jeju, Korea.
- 4Department of Family Medicine, Gangseo MizMedi Hospital, Seoul, Korea.
- 5Department of Family Medicine, Myongji Hospital, Kwandong University College of Medicine, Goyang, Korea.
- 6Department of Clinical Nursing Science, Yonsei University College of Nursing, Seoul, Korea.
- KMID: 2280715
- DOI: http://doi.org/10.4093/dmj.2013.37.2.132
Abstract
- BACKGROUND
Low levels of physical activity (PA) are strongly associated with the development of metabolic syndrome (MetS) and chronic diseases. However, few studies have examined this association in Koreans. The primary purpose of this study was to examine the associations between PA and MetS risks in Korean adults.
METHODS
A total of 1,016 Korean adults (494 males and 522 females) participated in this study. PA levels were assessed using the International PA Questionnaire. MetS risk factors were determined using clinically established diagnostic criteria.
RESULTS
Compared with the highest PA group, the group with the lowest level of PA was at greater risk of high triglyceride (TG) in males (odds ratio [OR], 1.87; 95% confidence interval [CI], 1.07 to 3.24) and of hemoglobin A1c > or =5.5% in females (OR, 1.75; 95% CI, 1.00 to 3.04) after adjusting for age and body mass index. Compared with subjects who met the PA guidelines, those who did not meet the guidelines were more likely to have low high density lipoprotein cholesterol in both males (OR, 1.69; 95% CI, 1.11 to 2.58), and females (OR, 1.82; 95% CI, 1.20 to 2.77). Furthermore, those who did not meet the PA guidelines were at increased risk of high TG levels in males (OR, 1.69; 95% CI, 1.23 to 2.86) and abnormal fasting glucose (OR, 1.93; 95% CI, 1.17 to 3.20) and MetS (OR, 2.10; 95% CI, 1.15 to 3.84) in females.
CONCLUSION
Increased levels of PA are significantly associated with a decreased risk of abnormal MetS components.
Keyword
MeSH Terms
Figure
-
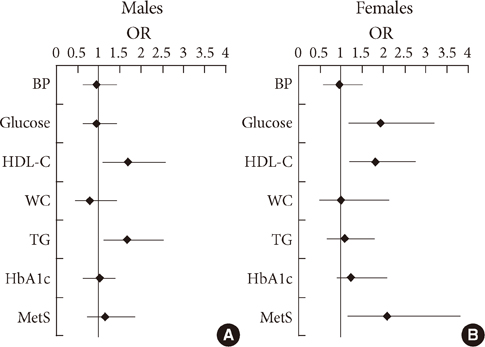
Fig. 1 Odd ratios (ORs) for metabolic syndrome (MetS) risk factors according to current physical activity (PA) recommendations. (A) Males. (B) Females. Adjusted for age and body mass index. Reference group: those who met the PA recommendations. BP, blood pressure; HDL-C, high density lipoprotein cholesterol; WC, waist circumference; TG, triglyceride; HbA1c, hemoglobin A1c.
Cited by 1 articles
-
Relationship between Physical Activity Level, Amount of Alcohol Consumption and Metabolic Syndrome in Korean Male Drinkers
Byung-Sung Kim, Myeong-Jin Kim, Hyun-Rim Choi, Cahng-Won Won, Sun-Young Kim
Korean J Sports Med. 2014;32(2):97-104. doi: 10.5763/KJSM.2014.32.2.97.
Reference
-
1. Hossain P, Kawar B, El Nahas M. Obesity and diabetes in the developing world: a growing challenge. N Engl J Med. 2007. 356:213–215.2. Adams KF, Schatzkin A, Harris TB, Kipnis V, Mouw T, Ballard-Barbash R, Hollenbeck A, Leitzmann MF. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006. 355:763–778.3. Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care. 2005. 28:1769–1778.4. Malik S, Wong ND, Franklin SS, Kamath TV, L'Italien GJ, Pio JR, Williams GR. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation. 2004. 110:1245–1250.5. LaMonte MJ, Barlow CE, Jurca R, Kampert JB, Church TS, Blair SN. Cardiorespiratory fitness is inversely associated with the incidence of metabolic syndrome: a prospective study of men and women. Circulation. 2005. 112:505–512.6. Wei M, Gibbons LW, Mitchell TL, Kampert JB, Lee CD, Blair SN. The association between cardiorespiratory fitness and impaired fasting glucose and type 2 diabetes mellitus in men. Ann Intern Med. 1999. 130:89–96.7. Laaksonen DE, Lakka HM, Salonen JT, Niskanen LK, Rauramaa R, Lakka TA. Low levels of leisure-time physical activity and cardiorespiratory fitness predict development of the metabolic syndrome. Diabetes Care. 2002. 25:1612–1618.8. Vaughan C, Schoo A, Janus ED, Philpot B, Davis-Lameloise N, Lo SK, Laatikainen T, Vartiainen E, Dunbar JA. The association of levels of physical activity with metabolic syndrome in rural Australian adults. BMC Public Health. 2009. 9:273.9. Boule NG, Haddad E, Kenny GP, Wells GA, Sigal RJ. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: a meta-analysis of controlled clinical trials. JAMA. 2001. 286:1218–1227.10. Lakka TA, Laaksonen DE. Physical activity in prevention and treatment of the metabolic syndrome. Appl Physiol Nutr Metab. 2007. 32:76–88.11. Nishida Y, Higaki Y, Tokuyama K, Fujimi K, Kiyonaga A, Shindo M, Sato Y, Tanaka H. Effect of mild exercise training on glucose effectiveness in healthy men. Diabetes Care. 2001. 24:1008–1013.12. Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011. 43:1334–1359.13. Korea Centers for Disease Control and Prevention. Korea National Health and Nutrition Examination Survey 2008. updated 2010 Apr 20. Available from: http://stat.mw.go.kr/stat/data/cm_data_view.jsp?menu_code=MN01010102&cont_seq=14245.14. Behavioral Risk Factor Surveillance System. 2009 Behavioral risk factor surveillance system report annual prevalence report. cited 2012 Nov 1. Available from: http://msdh.ms.gov/brfss/brfss2009ar.pdf.15. Wang J, Thornton JC, Russell M, Burastero S, Heymsfield S, Pierson RN Jr. Asians have lower body mass index (BMI) but higher percent body fat than do whites: comparisons of anthropometric measurements. Am J Clin Nutr. 1994. 60:23–28.16. Kadowaki T, Sekikawa A, Murata K, Maegawa H, Takamiya T, Okamura T, El-Saed A, Miyamatsu N, Edmundowicz D, Kita Y, Sutton-Tyrrell K, Kuller LH, Ueshima H. Japanese men have larger areas of visceral adipose tissue than Caucasian men in the same levels of waist circumference in a population-based study. Int J Obes (Lond). 2006. 30:1163–1165.17. Park YW, Allison DB, Heymsfield SB, Gallagher D. Larger amounts of visceral adipose tissue in Asian Americans. Obes Res. 2001. 9:381–387.18. Lee JW, Brancati FL, Yeh HC. Trends in the prevalence of type 2 diabetes in Asians versus whites: results from the United States National Health Interview Survey, 1997-2008. Diabetes Care. 2011. 34:353–357.19. Inoue M, Nakao M, Nomura K, Takeuchi T, Tsurugano S, Shinozaki Y, Yano E. Lack of leisure-time physical activity in non-obese Japanese men with components of metabolic syndrome. Tohoku J Exp Med. 2011. 223:269–276.20. Ma G, Luan D, Li Y, Liu A, Hu X, Cui Z, Zhai F, Yang X. Physical activity level and its association with metabolic syndrome among an employed population in China. Obes Rev. 2008. 9:Suppl 1. 113–118.21. Cho ER, Shin A, Kim J, Jee SH, Sung J. Leisure-time physical activity is associated with a reduced risk for metabolic syndrome. Ann Epidemiol. 2009. 19:784–792.22. Park HS, Oh SW, Cho SI, Choi WH, Kim YS. The metabolic syndrome and associated lifestyle factors among South Korean adults. Int J Epidemiol. 2004. 33:328–336.23. Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003. 35:1381–1395.24. Oh JY, Yang YJ, Kim BS, Kang JH. Validity and reliability of Korean version of international physical activity questionnaire (IPAQ) short form. J Korean Acad Fam Med. 2007. 28:532–541.25. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001. 285:2486–2497.26. Tan CE, Ma S, Wai D, Chew SK, Tai ES. Can we apply the National Cholesterol Education Program Adult Treatment Panel definition of the metabolic syndrome to Asians? Diabetes Care. 2004. 27:1182–1186.27. Ekelund U, Brage S, Franks PW, Hennings S, Emms S, Wareham NJ. Physical activity energy expenditure predicts progression toward the metabolic syndrome independently of aerobic fitness in middle-aged healthy Caucasians: the Medical Research Council Ely Study. Diabetes Care. 2005. 28:1195–1200.28. Franks PW, Ekelund U, Brage S, Wong MY, Wareham NJ. Does the association of habitual physical activity with the metabolic syndrome differ by level of cardiorespiratory fitness? Diabetes Care. 2004. 27:1187–1193.29. Jekal Y, Lee MK, Kim ES, Park JH, Lee HJ, Han SJ, Kang ES, Lee HC, Kim SH, Jeon JY. Effects of walking and physical activity on glucose regulation among type 2 diabetics. Korean Diabetes J. 2008. 32:60–67.30. Regitz-Zagrosek V, Lehmkuhl E, Weickert MO. Gender differences in the metabolic syndrome and their role for cardiovascular disease. Clin Res Cardiol. 2006. 95:136–147.31. Lee WY, Jung CH, Park JS, Rhee EJ, Kim SW. Effects of smoking, alcohol, exercise, education, and family history on the metabolic syndrome as defined by the ATP III. Diabetes Res Clin Pract. 2005. 67:70–77.32. Yoon YS, Oh SW, Baik HW, Park HS, Kim WY. Alcohol consumption and the metabolic syndrome in Korean adults: the 1998 Korean National Health and Nutrition Examination Survey. Am J Clin Nutr. 2004. 80:217–224.33. Kesaniemi YK, Danforth E Jr, Jensen MD, Kopelman PG, Lefebvre P, Reeder BA. Dose-response issues concerning physical activity and health: an evidence-based symposium. Med Sci Sports Exerc. 2001. 33:6 Suppl. S351–S358.34. Kim ES, Han SM, Kim YI, Song KH, Kim MS, Kim WB, Park JY, Lee KU. Prevalence and clinical characteristics of metabolic syndrome in a rural population of South Korea. Diabet Med. 2004. 21:1141–1143.35. Kim DM, Ahn CW, Nam SY. Prevalence of obesity in Korea. Obes Rev. 2005. 6:117–121.36. Kim S, Moon S, Popkin BM. The nutrition transition in South Korea. Am J Clin Nutr. 2000. 71:44–53.37. Rennie KL, Wareham NJ. The validation of physical activity instruments for measuring energy expenditure: problems and pitfalls. Public Health Nutr. 1998. 1:265–271.38. Shephard RJ. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med. 2003. 37:197–206.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison between walking and moderate-to-vigorous physical activity: associations with metabolic syndrome components in Korean older adults
- Prevalence and Influencing Factors of Metabolic Syndrome Among Persons with Physical Disabilities
- Relationship between Change in Physical Activity and Risk of Metabolic Syndrome: A Prospective Cohort Study
- The Association between the Type and Level of Physical Activity and Metabolic Syndrome in Korean Adults Aged 40 Years and over: Results from the Eighth Korea National Health and Nutrition Examination Survey (2019–2021)
- Fasting Plasma Glucose Levels and Metabolic Syndrome in Normoglycemic Adults
