Clin Exp Otorhinolaryngol.
2012 Mar;5(1):1-9.
Characteristics of Nasal Resonance and Perceptual Rating in Prelingual Hearing Impaired Adults
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hongsh@skku.edu
- 2Graduate Program in Speech & Language Pathology, Yonsei University, Seoul, Korea.
- 3Department of Communication Disorders, Korea Nazarene University, Cheonan, Korea.
- 4Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 5Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea. pes1234@yuhs.ac
Abstract
OBJECTIVES
Resonance problems in hearing impaired (HI) individuals have been described as aspects of nasality. However, there are limitations in being able to explain the range of resonance problems. Therefore, this study suggests a perceptual rating that will effectively explain the characteristics of resonance problems in HI individuals.
METHODS
Nasalance scores were obtained from 32 subjects in each of HI and normal hearing (NH) groups using a nasometer. The subjects were categorized into groups based on normal and abnormal nasalance ranges. The abnormal nasalance range group was further divided into hyper-, hypo-, and mixed-nasal groups. Nasalance scores were based the individuals performance in a series of passage and syllable tasks. The perceptual rating was evaluated using a newly introduced tool, 'vertical focus of resonance' (VFR), which focuses on the resonance energy in the frontal, throat, pharyngeal and nasal locations.
RESULTS
The NH group demonstrated a significantly lower nasalance score in the oral coupling and passage tasks than the HI group. Based on the results of nasalance correlation analysis, the HI group showed highly significant correlations between syllable and passage tasks, as contrasted with the NH group. There were significant differences in VFR between the nasalance types in both the NH and the HI groups.
CONCLUSION
The HI hyper-nasal group showed tendencies of velopharyngeal opening, as opposed to the HI hypo-nasal group which showed tendencies of velopharyngeal closure. The HI mixed-nasal group showed inappropriate coordination of velopharyngeal function. In the HI group, the results of VFR showed that the air flow and the resonance energy were not released from the cavity of resonance. The suggested VFR tool explains the focusing characteristics of resonance energy within a continuation of speech sound regardless of the phonetic environment. Therefore, VFR may be a useful tool in explaining the deviant resonance patterns of HI individuals.
Keyword
Figure
-
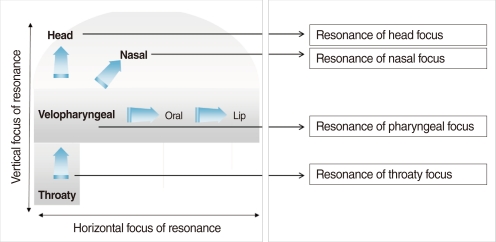
Fig. 1 Focus of resonance and aspects of deviant resonance.
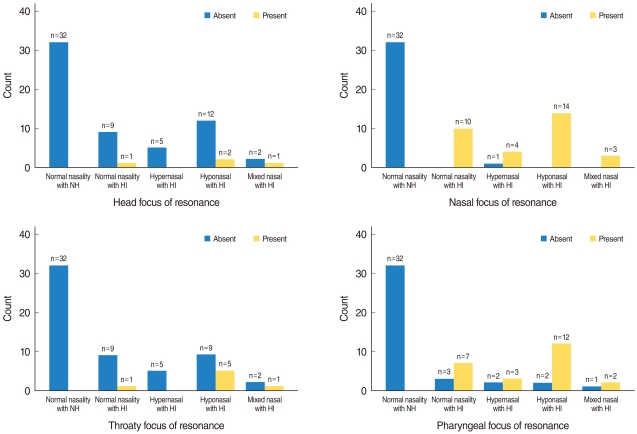
Fig. 2 Vertical focus of resonance for each nasalance type. NH, normal hearing subjects; HI, hearing impaired subjects.
Reference
-
1. Evans MK, Deliyski DD. Acoustic voice analysis of prelingually deaf adults before and after cochlear implantation. J Voice. 2007; 11. 21(6):669–682. PMID: 16952440.
Article2. Fletcher SG, Mahfuzh F. Nasalance in the speech of children with normal hearing and children with hearing loss. Am J Speech Lang Pathol. 1999; 8. 8(3):241–248.
Article3. Goffman L, Ertmer DJ, Erdle C. Changes in speech production in a child with a cochlear implant: acoustic and kinematic evidence. J Speech Lang Hear Res. 2002; 10. 45(5):891–901. PMID: 12381047.4. Seifert E, Oswald M, Bruns U, Vischer M, Kompis M, Haeusler R. Changes of voice and articulation in children with cochlear implants. Int J Pediatr Otorhinolaryngol. 2002; 11. 11. 66(2):115–123. PMID: 12393244.
Article5. Boone DR, McFarlane SC, von Berg SL. The voice and voice therapy. 2005. 7th ed. Boston, MA: Pearson/Allyn & Bacon.6. Kay Elemetrics Co. Nasometer II model 6400: installation, operations and maintenance manual, issue C. 2003. Lincoln Park, NJ: Kay Elemetrics Co..7. Higgins MB, McCleary EA, Ide-Helvie DL, Carney AE. Speech and voice physiology of children who are hard of hearing. Ear Hear. 2005; 12. 26(6):546–558. PMID: 16377992.
Article8. Fletcher SG, Daly DA. Nasalance in utterances of hearing-impaired speakers. J Commun Disord. 1976; 3. 9(1):63–73. PMID: 965505.
Article9. LaPine PR, Stewart MG, Tatchell J. Application of nasometry to speech samples of hearing-impaired children. Percept Mot Skills. 1991; 10. 73(2):467–475. PMID: 1766773.
Article10. Lock RB, Seaver EJ 3rd. Nasality and velopharyngeal function in five hearing impaired adults. J Commun Disord. 1984; 2. 17(1):47–64. PMID: 6715568.
Article11. Andrews ML. Manual of voice treatment: pediatrics through geriatrics. 1995. San Diego, CA: Singular Publishing.12. McClumpha SL. Cinefluorographic investigation of velopharyngeal function in selected deaf speakers. Folia Phoniatr (Basel). 1969; 21(5):368–374. PMID: 5371458.
Article13. Higgins MB, McCleary EA, Carney AE, Schulte L. Longitudinal changes in children's speech and voice physiology after cochlear implantation. Ear Hear. 2003; 2. 24(1):48–70. PMID: 12598813.
Article14. Park MK, Lee EK, Yu SC, Koh KS, Kim BJ, Baek RM. Nasalance scores in normal Koreans. 65th American Cleft Palate-Craniofacial Association Annual Meetings. 2008 April 14-18; Philadelphia, PA, USA.15. Van Lierde KM, Vinck BM, Baudonck N, De Vel E, Dhooge I. Comparison of the overall intelligibility, articulation, resonance, and voice characteristics between children using cochlear implants and those using bilateral hearing aids: a pilot study. Int J Audiol. 2005; 8. 44(8):452–465. PMID: 16149240.
Article16. Vallino-Napoli LD, Montgomery AA. Examination of the standard deviation of mean nasalance scores in subjects with cleft palate: implications for clinical use. Cleft Palate Craniofac J. 1997; 11. 34(6):512–519. PMID: 9431469.
Article17. Kummer AW. Cleft palate and craniofacial anomalies: effects on speech and resonance. 2008. Clifton Park, NY: Thomson Delmar Learning.18. Hardin MA, Van Demark DR, Morris HL, Payne MM. Correspondence between nasalance scores and listener judgments of hypernasality and hyponasality. Cleft Palate Craniofac J. 1992; 7. 29(4):346–351. PMID: 1643065.
Article19. Dotevall H, Ejnell H, Bake B. Nasal airflow patterns during the velopharyngeal closing phase in speech in children with and without cleft palate. Cleft Palate Craniofac J. 2001; 7. 38(4):358–373. PMID: 11420016.
Article20. Shakespeare W. The art of singing. 1921. Boston: Oliver Ditson.21. Nguyen LH, Allegro J, Low A, Papsin B, Campisi P. Effect of cochlear implantation on nasality in children. Ear Nose Throat J. 2008; 3. 87(3):138140–143. PMID: 18404908.
Article22. Peterson-Falzone SJ, Hardin-Jones MA, Karnell MP, McWilliams BJ. Cleft palate speech. 2001. St. Louis: Mosby.23. Leeper HA, Tissington ML, Munhall KG. Temporal characteristics of velopharyngeal function in children. Cleft Palate Craniofac J. 1998; 5. 35(3):215–221. PMID: 9603555.
Article24. Peterson-Falzone SJ, Trost-Cardamone J, Karnell MP, Hardin-Jones MA. Chapter 3, Effects of cleft and non-cleft VPI on speech in older children. The clinician's guide to treating cleft palate speech. 2006. St. Louis: Mosby;p. 17–40.25. Dotevall H, Lohmander-Agerskov A, Almquist SA, Bake B. Aerodynamic assessment of velopharyngeal function during normal speech containing different places of articulation. Folia Phoniatr Logop. 1998; 50(2):53–63. PMID: 9624856.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adaptation and Validation of the Perceptual Performance Test in Malayalam
- Educational Status in Bilateral Prelingual Deaf Children with Cochlear Implantation
- Substitution Patterns of Phoneme Errors in Hearing Aid and Cochlear Implant Users
- Cortical Auditory Evoked Potential in Adults With Cochlear Implants: A Comparison With Adults With Normal Hearing
- Translation, Adaptation and Cross-Cultural Validation of Hearing Handicap Inventory for Adult in Malay Language
