Anatomical Analysis of Intraorbital Structures Regarding Sinus Surgery Using Multiplanar Reconstruction of Computed Tomography Scans
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, The Catholic University of Korea College of Medicine, Seoul, Korea. entkjm@catholic.ac.kr
Abstract
OBJECTIVES
This study aimed to investigate the anatomy of the intraorbital structures regarding to endoscopic sinus surgery and external frontal sinus surgery analyzing computer tomography (CT) scans.
METHODS
The CT scans of 100 patients were retrospectively evaluated. The anatomic relationships between the intraorbital structures and paranasal structures were measured using multiplanar reconstruction of the CT scan.
RESULTS
The mean distances from the medial orbital floor (MOF) to the intraorbital structures were measured at the depth of the anterior ethmoid (AE), basal lamella (BL), and midportion of posterior ethmoid (PE) in the coronal planes respectively. The mean distances from the MOF to the medial rectus muscle and inferior rectus muscle at the depth of AE were approximately 8 mm and those distances in the BL and PE decreased rapidly. The mean distances from the MOF to the infraorbital nerve at the depth of the AE and BL were approximately more than 10 mm. The mean distances from the vertical axis, which passed through the MOF, to the superior oblique muscle and optic nerve at the depth of the PE were approximately 5 mm medially and 1 mm laterally. In addition, the mean distance from the midline to the trochlea of the superior oblique muscle was approximately 15 mm.
CONCLUSIONS
Those measurements provide spatial information on the placements of the extraocular muscles within the orbit. The measurements will contribute to the avoidance of orbital complications during sinus surgery.
Keyword
MeSH Terms
Figure
-
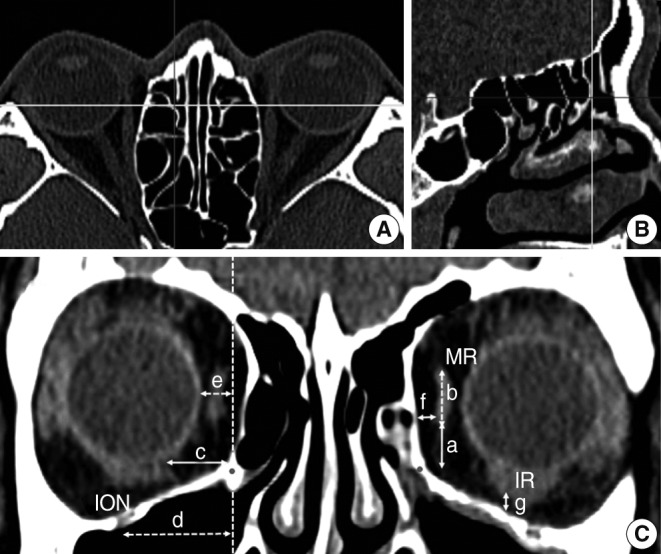
Fig. 1 Multiplanar reconstruction of the computed tomography scan and measurements regarding the intraorbital structures at the depth of the AE. The AE (yellow line) was identified in the axial plane (A) and sagittal plane (B). The red line in the axial plane meant the position of the sagittal plane and the blue line in the sagittal plane meant the level of the axial plane. The relationship between the intraorbital structures and the references points at the depth of the AE were measured in the coronal plane (C). (a) vertical distance from the MOF to the inferior margin of the MR; (b) vertical diameter of the MR; (c) horizontal distances from the MOF to the medial margin of the IR; (d) horizontal distances from the vertical axis of MOF to the ION; (e) horizontal distance from the vertical axis of the MOF to the orbit ball; (f) shortest horizontal distance from the lamina papyracea to the MR; (g) shortest vertical distance from the orbital floor to the IR. AE, anterior wall of the ethmoid bulla; MOF, medial orbital floor (red point); MR, medial rectus muscle; IR, inferior rectus muscle; ION, infraorbital nerve; dashed vertical line, the vertical axis of the MOF.
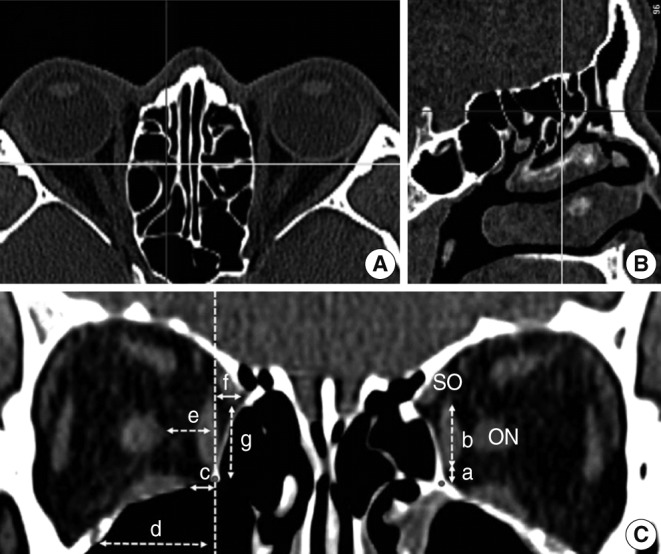
Fig. 2 Multiplanar reconstruction of the computed tomography scan and measurements regarding the intraorbital structures at the depth of the BL. The BL (yellow line) was identified in the axial plane (A) and sagittal plane (B). The red line in the axial plane meant the position of the sagittal plane and the blue line in the sagittal plane meant the level of the axial plane. The relationship between intraorbital structures and the reference points at the depth of the BL were measured in the coronal plane (C). The distances (a-d) were measured at the depth of BL using identical landmarks to the distances in Fig. 1. The distance (e) was the horizontal distance from the vertical axis of the MOF to the ON. The distance (f) was the horizontal distance from the vertical axis of the MOF to the medial margin of the SO and the distance (g) was the vertical distance from the MOF to the inferior margin of the SO. BL, basal lamella; MOF, medial orbital floor, red point; SO, superior oblique muscle; ON, optic nerve; dashed vertical line, the vertical axis of the MOF.
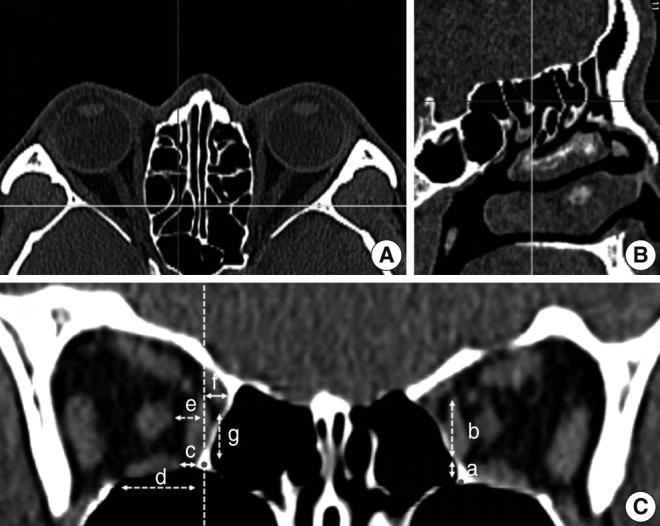
Fig. 3 Multiplanar reconstruction of the computed tomography scan and measurements regarding the intraorbital structures at the depth of the PE. The PE (yellow line) was identified in the axial plane (A) and sagittal plane (B). The red line in the axial plane meant the position of the sagittal plane and the blue line in the sagittal plane meant the level of the axial plane. The relationship between intraorbital structures and the reference points at the depth of the PE were measured in the coronal plane (C). The distances (a-g) were measured at the depth of the PE using identical landmarks to the distances in Fig. 2. PE, midportion of posterior ethmoid; red point, medial orbital floor (MOF); dashed vertical line, the vertical axis of the MOF.
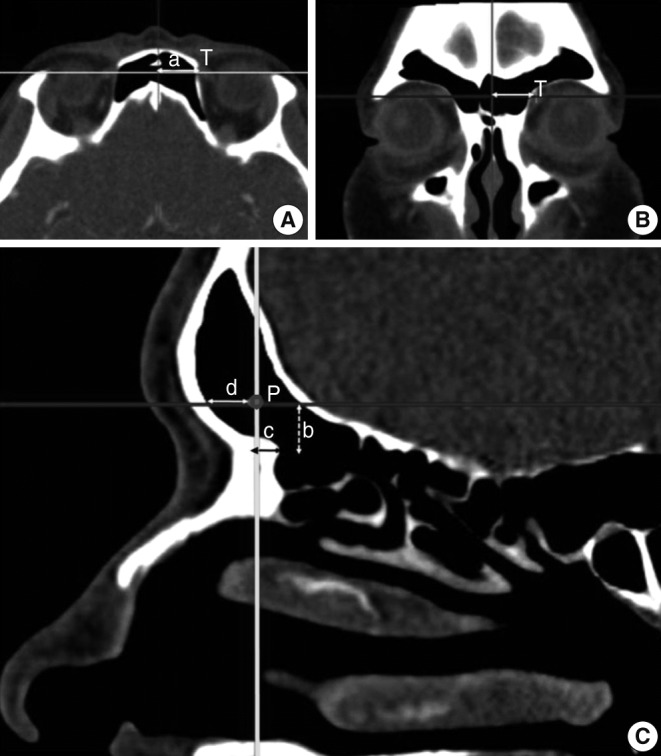
Fig. 4 Multiplanar reconstruction of the computed tomography scan and measurements regarding the trochlea of the SO. To evaluate the relationship between the surrounding structures and the trochlea, the coronal, axial, and parasagittal planes were observed. The red line and yellow line in the axial plane meant the position of the sagittal plane and coronal plane separately and the blue line in the coronal plane meant the level of the axial plane. The distance (a) was the horizontal distance between the midline and trochlea and well identified in axial (A) and coronal (B) planes. In the parasagittal plane (C) that was located at the midpoint of the frontal sinus opening, an imaginary point (P) that was parallel to the trochlea in position and level was drawn. The distance (b) was the vertical distance from P to the frontal beak. The distances (c) and (d) were the anteroposterior distances from P to the anterior frontal sinus wall and frontal beak, separately. SO, superior oblique muscle; T, trochlea.
Reference
-
1. Khalil HS, Eweiss AZ, Clifton N. Radiological findings in patients undergoing revision endoscopic sinus surgery: a retrospective case series study. BMC Ear Nose Throat Disord. 2011; 5. 11:4. PMID: 21548971.
Article2. Bhatti MT, Giannoni CM, Raynor E, Monshizadeh R, Levine LM. Ocular motility complications after endoscopic sinus surgery with powered cutting instruments. Otolaryngol Head Neck Surg. 2001; 11. 125(5):501–509. PMID: 11700450.
Article3. Kim HJ, Kim CH, Song MS, Yoon JH. Diplopia secondary to endoscopic sinus surgery. Acta Otolaryngol. 2004; 12. 124(10):1237–1239. PMID: 15768826.
Article4. Han JK, Higgins TS. Management of orbital complications in endoscopic sinus surgery. Curr Opin Otolaryngol Head Neck Surg. 2010; 2. 18(1):32–36. PMID: 19935067.
Article5. Bartley J, Eagleton N, Rosser P, Al-Ali S. Superior oblique muscle palsy after frontal sinus mini-trephine. Am J Otolaryngol. 2012; Jan-Feb. 33(1):181–183. PMID: 21696855.
Article6. Casiano RR. A stepwise surgical technique using the medial orbital floor as the key landmark in performing endoscopic sinus surgery. Laryngoscope. 2001; 6. 111(6):964–974. PMID: 11404605.
Article7. Ozgen A, Ariyurek M. Normative measurements of orbital structures using CT. AJR Am J Roentgenol. 1998; 4. 170(4):1093–1096. PMID: 9530066.
Article8. Ela-Dalman N, Velez FG, Rosenbaum AL. Importance of sagittal orbital imaging in evaluating extraocular muscle trauma following endoscopic sinus surgery. Br J Ophthalmol. 2006; 6. 90(6):682–685. PMID: 16488930.
Article9. Sheikh M, Abalkhail S, Doi SA, Al-Shoumer KA. Normal measurement of orbital structures: implications for the assessment of Graves' ophthalmopathy. Australas Radiol. 2007; 6. 51(3):253–256. PMID: 17504317.
Article10. Lee JS, Lim DW, Lee SH, Oum BS, Kim HJ, Lee HJ. Normative measurements of Korean orbital structures revealed by computerized tomography. Acta Ophthalmol Scand. 2001; 4. 79(2):197–200. PMID: 11284763.
Article11. Thacker NM, Velez FG, Demer JL, Wang MB, Rosenbaum AL. Extraocular muscle damage associated with endoscopic sinus surgery: an ophthalmology perspective. Am J Rhinol. 2005; Jul-Aug. 19(4):400–405. PMID: 16171176.
Article12. Karaki M, Kobayashi R, Kobayashi E, Ishii G, Kagawa M, Tamiya T, et al. Computed tomographic evaluation of anatomic relationship between the paranasal structures and orbital contents for endoscopic endonasal transethmoidal approach to the orbit. Neurosurgery. 2008; 7. 63(1 Suppl 1):ONS15–ONS19. PMID: 18728593.
Article13. Schaefer SD. An anatomic approach to endoscopic intranasal ethmoidectomy. Laryngoscope. 1998; 11. 108(11 Pt 1):1628–1634. PMID: 9818817.
Article14. Boopathi S, Chakravarthy Marx S, Dhalapathy SL, Anupa S. Anthropometric analysis of the infraorbital foramen in a South Indian population. Singapore Med J. 2010; 9. 51(9):730–735. PMID: 20938615.15. Wee DT, Carney AS, Thorpe M, Wormald PJ. Endoscopic orbital decompression for Graves' ophthalmopathy. J Laryngol Otol. 2002; 1. 116(1):6–9. PMID: 11860643.
Article16. Isaacs SJ, Goyal P. Endoscopic anatomy of the pterygopalatine fossa. Am J Rhinol. 2007; Sep-Oct. 21(5):644–647. PMID: 17999806.
Article17. Chastain JB, Sindwani R. Anatomy of the orbit, lacrimal apparatus, and lateral nasal wall. Otolaryngol Clin North Am. 2006; 10. 39(5):855–864. PMID: 16982251.
Article18. Dallan I, Seccia V, Lenzi R, Castelnuovo P, Bignami M, Battaglia P, et al. Transnasal approach to the medial intraconal space: anatomic study and clinical considerations. Minim Invasive Neurosurg. 2010; 8. 53(4):164–168. PMID: 21132607.
Article19. Hwang HS, Park MK, Lee WJ, Cho JH, Kim BK, Wilkinson CM. Facial soft tissue thickness database for craniofacial reconstruction in Korean adults. J Forensic Sci. 2012; 11. 57(6):1442–1447. PMID: 22621203.
Article20. Agthong S, Huanmanop T, Chentanez V. Anatomical variations of the supraorbital, infraorbital, and mental foramina related to gender and side. J Oral Maxillofac Surg. 2005; 6. 63(6):800–804. PMID: 15944977.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Sphenoid Sinus and Surrounding Structures Using Multidetector Computed Tomography
- Feasibility and Safety of Superolateral Sphenoidotomy: Radiologic Study by Analyzing Multiplanar Reconstructive CT Scans
- Three-dimensional linear and volumetric computed tomography analysis of the frontal sinus
- Evaluation of Localized Aortic Dissection at Sinus of Valsalva by Coronary CT Angiography with Multiplanar Reformation: A Case Report
- The Anatomical Relationship between the Anterior Ethmoid Artery, Frontal Sinus, and Intervening Air Cells; Can the Artery Be Useful Landmark?
