Clin Exp Otorhinolaryngol.
2013 Dec;6(4):269-271.
Gossypiboma of the Neck Mimicking an Isolated Neck Recurrence
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Inha University School of Medicine, Incheon, Korea. ymk416@inha.ac.kr
Abstract
- A gossypiboma (also called textiloma or retained surgical sponge) of the neck is rarely reported compared to intraabdominal or intrathoracic gossypibomas and also can be misdiagnosed as metastatic lymph nodes. A patient was referred to our clinic for a supraclavicular neck mass 6 months after thyroidectomy and neck dissection for papillary thyroid carcinoma in another hospital. It was initially considered an isolated neck recurrence, but it was finally diagnosed as gossypiboma by a pathological examination of the surgically-excised specimen. Characteristic findings of computed tomography or positron emission tomography/computed tomography might be helpful to differentiate the gossypiboma from malignant neck mass or other inflammatory conditions. It is essential for clinicians to be aware of this disease entity in differential diagnosis of neck recurrence because a gossypiboma in the neck can be misinterpreted as a malignancy to induce unwarranted radical surgery.
Keyword
MeSH Terms
Figure
-
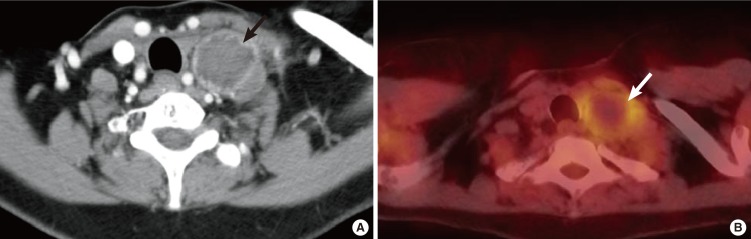
Fig. 1 The radiologic findings of retained gauze. (A) Neck computed tomography (CT) shows a low attenuating homogenous central mass with a hyperdense, well-enhancing, irregular rim. (B) Positron emission tomography/CT depicts the hot uptake on the rim of the left supraclavicular mass and no uptake on internal area of mass.
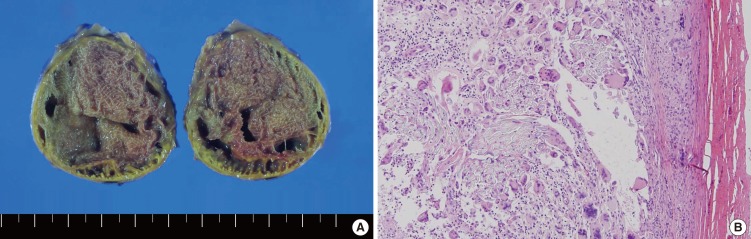
Fig. 2 (A) Cross section view. The specimen shows retained gauze with external capsule formation. (B) Microscopic examination revealed a foreign body with dense fibrocystic wall with a lining of multinucleated giant cells. Chronic inflammatory cell infiltrations were also visible around the foreign body (H&E, ×100).
Reference
-
1. Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2003; 1. 348(3):229–235. PMID: 12529464.
Article2. Lauwers PR, Van Hee RH. Intraperitoneal gossypibomas: the need to count sponges. World J Surg. 2000; 5. 24(5):521–527. PMID: 10787070.
Article3. Park HJ, Im SA, Chun HJ, Park SH, O JH, Lee KY. Changes in CT appearance of intrathoracic gossypiboma over 10 years. Br J Radiol. 2008; 2. 81(962):e61–e63. PMID: 18238918.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intracranial Gossypiboma Mimicking a Recurrent Low Grade Astrocytoma: Case Report
- Pathologic Fracture of Femoral Neck due to Mass suspicious of Gossypiboma in Proximal Thigh: Case Report
- A Case of Gossypiboma Associated with Xanthogranulomatous Inflammation
- A Case of Gossypiboma in the Peritonsillar Space
- Gossypiboma in the Neck after Total Thyroidectomy: A Case Report
