Korean J Pain.
2012 Oct;25(4):267-271. 10.3344/kjp.2012.25.4.267.
Pain and Anxiety Management in Minimally Invasive Repair of Pectus Excavatum
- Affiliations
-
- 1Department of Pediatric Surgery, Children's Hospital A. Meyer, Florence, Italy.
- 2Pain Control Team, Children's Hospital A. Meyer, Florence, Italy. a.messeri@meyer.it
- 3Department of Pediatrics - Surgery Unit, Le Scotte Hospital, Siena, Italy.
- KMID: 2278169
- DOI: http://doi.org/10.3344/kjp.2012.25.4.267
Abstract
- The Nuss procedure for the correction of Pectus Excavatum (PE) is associated with intense postoperative pain. Our strategy to control early postoperative pain is to combine epidural with intravenous analgesia. Our aim was to analyse our pain control strategy by reviewing all the PE cases treated at our institution. Sixty consecutive patients, aged between 12 and 26 years old, received the PE operation at our institution from January, 2007 to September, 2010. The median age was 16 (12-27) with a male/female ratio of about 7/1. An epidural catheter was employed in all the cases, with 38 patients (63%) requiring additional drugs to control pain, which remained in place for 74 hours (72-96). The pain score was higher in male patients, but lower in those younger than 16 years old. Moreover, patients that consumed benzodiazepines had a significant decrease in cumulative opioid intake (P = 0.0408). Both gender and age had an impact on pain control, while we noticed a synergistic effect between opiates and tranquillizers.
Keyword
MeSH Terms
Figure
-
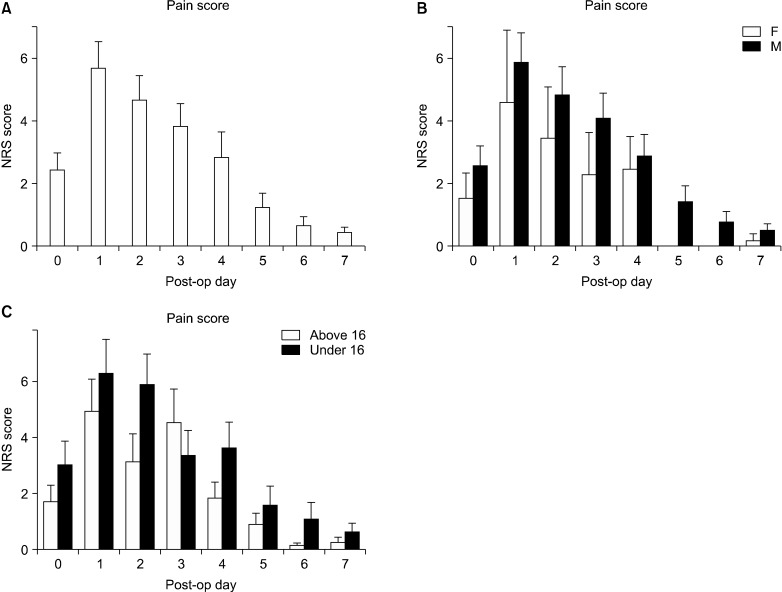
Fig. 1 The figure shows the average pain experienced by patients during the first 7 postoperative days (A), divided by gender (B), divided in two age groups (C).
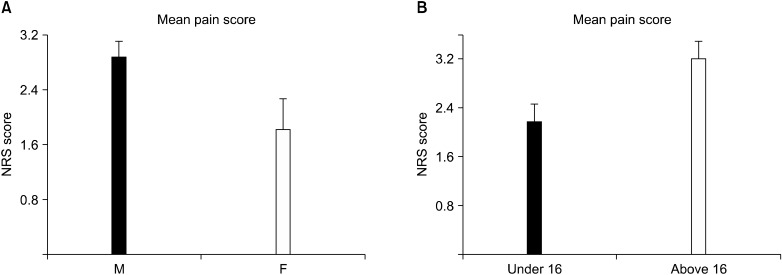
Fig. 2 The figure shows the mean pain experienced by patients in the post operative period divided by gender (A) P = 0.0417, divided in two age groups (B) P = 0.0199.
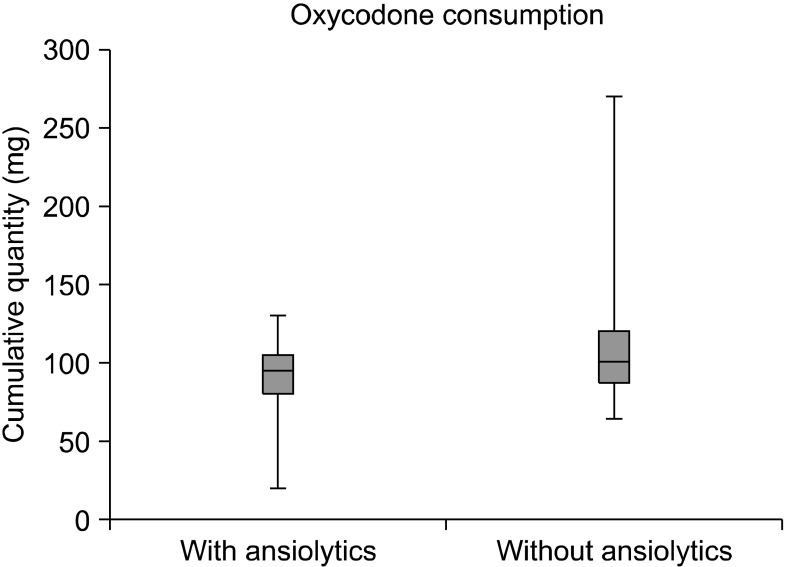
Fig. 3 The figure shows the different opoid consumption in two groups. Patients who assumed benzodiazepines had a significant decreased oxycodone intake (P = 0.0408).
Reference
-
1. Grosen K, Pfeiffer-Jensen M, Pilegaard HK. Postoperative consumption of opioid analgesics following correction of pectus excavatum is influenced by pectus severity: a single-centre study of 236 patients undergoing minimally invasive correction of pectus excavatum. Eur J Cardiothorac Surg. 2010; 37:833–839. PMID: 19853467.
Article2. Rugyte DC, Kilda A, Karbonskiene A, Barauskas V. Systemic postoperative pain management following minimally invasive pectus excavatum repair in children and adolescents: a retrospective comparison of intravenous patient-controlled analgesia and continuous infusion with morphine. Pediatr Surg Int. 2010; 26:665–669. PMID: 20490811.
Article3. St Peter SD, Weesner KA, Sharp RJ, Sharp SW, Ostlie DJ, Holcomb GW 3rd. Is epidural anesthesia truly the best pain management strategy after minimally invasive pectus excavatum repair? J Pediatr Surg. 2008; 43:79–82. PMID: 18206460.
Article4. Futagawa K, Suwa I, Okuda T, Kamamoto H, Sugiura J, Kajikawa R, et al. Anesthetic management for the minimally invasive Nuss procedure in 21 patients with pectus excavatum. J Anesth. 2006; 20:48–50. PMID: 16421678.
Article5. Weber T, Mätzl J, Rokitansky A, Klimscha W, Neumann K, Deusch E, et al. Superior postoperative pain relief with thoracic epidural analgesia versus intravenous patientcontrolled analgesia after minimally invasive pectus excavatum repair. J Thorac Cardiovasc Surg. 2007; 134:865–870. PMID: 17903498.
Article6. Soliman IE, Apuya JS, Fertal KM, Simpson PM, Tobias JD. Intravenous versus epidural analgesia after surgical repair of pectus excavatum. Am J Ther. 2009; 16:398–403. PMID: 19262363.
Article7. Cucchiaro G, Adzick SN, Rose JB, Maxwell L, Watcha M. A comparison of epidural bupivacaine-fentanyl and bupivacaine-clonidine in children undergoing the Nuss procedure. Anesth Analg. 2006; 103:322–327. PMID: 16861412.
Article8. Walaszczyk M, Knapik P, Misiolek H, Korlacki W. Epidural and opioid analgesia following the Nuss procedure. Med Sci Monit. 2011; 17:PH81–PH86. PMID: 22037752.
Article9. Densmore JC, Peterson DB, Stahovic LL, Czarnecki ML, Hainsworth KR, Davies HW, et al. Initial surgical and pain management outcomes after Nuss procedure. J Pediatr Surg. 2010; 45:1767–1771. PMID: 20850618.
Article10. Yapici D, Atici S, Alic M, Ayan E, Koksel O. Morphine added to local anaesthetic improves epidural analgesia in minimally invasive Nuss operation for pectus excavatum. Br J Anaesth. 2008; 100:280. PMID: 18212003.
Article11. Al-Assiri A, Kravarusic D, Wong V, Dicken B, Milbrandt K, Sigalet DL. Operative innovation to the "Nuss" procedure for pectus excavatum: operative and functional effects. J Pediatr Surg. 2009; 44:888–892. PMID: 19433163.
Article12. Reinoso-Barbero F, Fernández A, Durán P, Castro LE, Campo G, Melo MM. Thoracic epidural analgesia vs patientcontrolled analgesia with intravenous fentanyl in children treated for pectus excavatum with the Nuss procedure. Rev Esp Anestesiol Reanim. 2010; 57:214–219. PMID: 20499799.
Article13. Butkovic D, Kralik S, Matolic M, Kralik M, Toljan S, Radesic L. Postoperative analgesia with intravenous fentanyl PCA vs epidural block after thoracoscopic pectus excavatum repair in children. Br J Anaesth. 2007; 98:677–681. PMID: 17363405.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous Nuss Operation and Mammoplasty in an Adult Patient with Pectus Excavatum: A case report
- Minimally Invasive Simultaneous Treatment for Congenital Cystic Adenomatoid Malformation associated with Pectus Excavatum : A case report
- Early Results of the Nuss Procedure
- Repair of Recurrent Pectus Excavatum with a Huge Chest Wall Defect in a Patient with a Previous Ravitch and Pectus Bar Repair: A Case Report
- Serratus Anterior Plane Block: A Better Modality of Pain Control after Pectus Excavatum Repair
