Three-dimensional evaluation of the relationship between nasopharyngeal airway shape and adenoid size in children
- Affiliations
-
- 1Department of Orthodontics, Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea. dentpark64@hanmail.net
- 2Departmet of Clinical Orthodontics, Graduate School of Hallym University, Chuncheon, Korea.
- KMID: 2272251
- DOI: http://doi.org/10.4041/kjod.2013.43.4.160
Abstract
OBJECTIVE
To evaluate the shapes and sizes of nasopharyngeal airways by using cone-beam computed tomography and to assess the relationship between nasopharyngeal airway shape and adenoid hypertrophy in children.
METHODS
Linear and cross-sectional measurements on frontal and sagittal cross-sections containing the most enlarged adenoids and nasopharyngeal airway volumes were obtained from cone-beam computed tomography scans of 64 healthy children (11.0 +/- 1.8 years), and the interrelationships of these measurements were evaluated.
RESULTS
On the basis of frontal section images, the subjects' nasopharyngeal airways were divided into the following 2 types: the broad and long type and the narrow and flat type. The nasopharyngeal airway sizes and volumes were smaller in subjects with narrow and flat airways than in those with broad and long airways (p < 0.01). Children who showed high adenoid-nasopharyngeal ratios on sagittal imaging, indicating moderate to severe adenoid hypertrophy, had the narrow and flat type nasopharyngeal airway (p < 0.01).
CONCLUSIONS
Cone-beam computed tomography is a clinically simple, reliable, and noninvasive tool that can simultaneously visualize the entire structure and a cross section of the nasopharyngeal airway and help in measurement of adenoid size as well as airway volume in children with adenoid hypertrophy.
Keyword
Figure
-
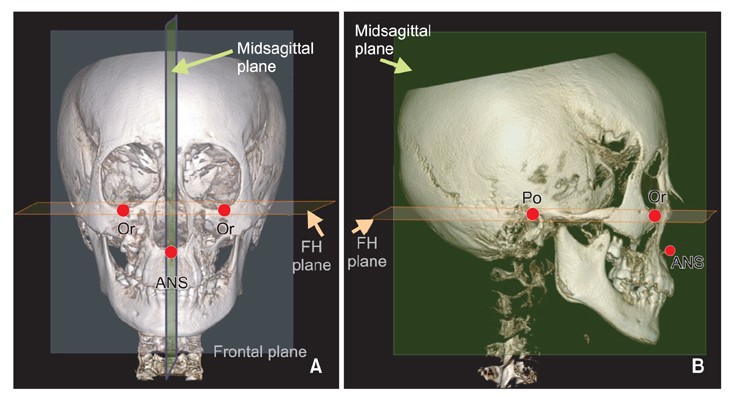
Figure 1 Three-dimensional cone-beam computed tomography images were reoriented, based on the Frankfurt (FH) plane (the FH plane is passing through the right porion [Po] and the left and right orbitales [Or]) and the anterior nasal spine (ANS) used in this study. The FH plane was defined as the standard horizontal plane. The midsagittal plane is perpendicular to the FH plane and includes the ANS. A frontal plane, including the right and left orbitales, is also perpendicular to the FH plane and the sagittal plane. A, Frontal view of a skull. B, Sagittal view of a skull.
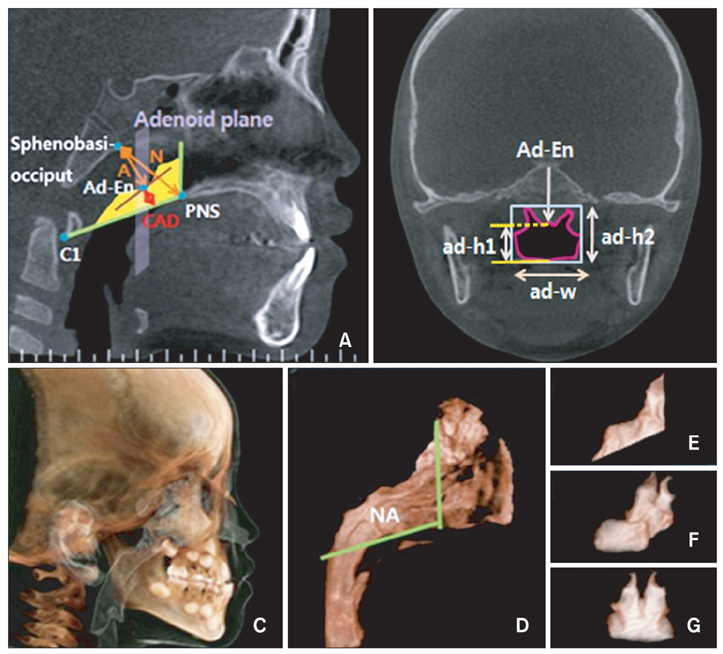
Figure 2 Three-dimensional (3D) measurements of the nasopharyngeal airway on the adenoid plane in this study. A, The nasopharyngeal airway on the midsagittal view. The most enlarged adenoid was tangential; the nasopharyngeal airway's narrowest part is identified as Ad-En; and the nasopharyngeal airway is shown as the yellow area. B, The cross-sectional image of the nasopharyngeal airway in the frontal plane, in which the most enlarged adenoid was included (adenoid plane). C, The volumetric image of the skeletal and internal soft tissues. D, The volumetric image of the pharyngeal airway; the nasopharyngeal airway is shown within the boundary indicated by the green line. E, 3D image of the nasopharyngeal airway in the sagittal view of Figure 2D. F, 3D image of the nasopharyngeal airway in the superolateral view of Figure 2D. G, 3D image of the nasopharyngeal airway in the frontal view of Figure 2D. CAD, Convex adenoid distance; PNS, posterior nasal spine; NA, nasopharyngeal airway; A, the distance between the outermost point of convexity of adenoid shadow and sphenobasiocciput; N, the distance between sphenobasiocciput and posterior end of the hard palate.
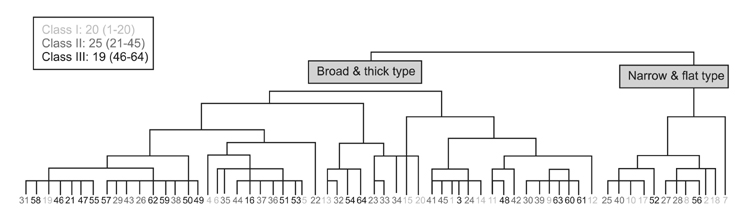
Figure 3 Dendrogram of the 2 nasopharyngeal airway cross-sectional shapes in the adenoid plane by a cluster analysis; the broad and thick (BT)-shaped airway group and the narrow and flat (NF)-shaped airway group. In our study, 52 of the 64 (81.2%) subjects belonged to the BT group, and 12 of the 64 (18.8%) subjects belonged to the NF group.
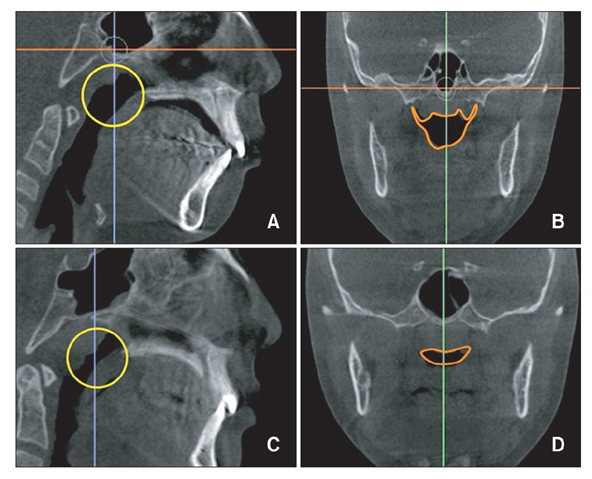
Figure 4 Examples of the 2 types of nasopharyngeal airway shapes. Preadolescents who have left-to-right enlarged adenoids on the adenoid plane were more likely to show the narrow and flat (NF) shaped airways to a significant degree and have more flat superior borders and relatively small nasopharyngeal airway spaces; their nasopharyngeal airways demonstrated shorter distances from the superior to inferior borders of their nasopharyngeal airways on the adenoid plane. A, Relatively large nasopharyngeal airway in the sagittal plane. B, Broad and thick type nasopharyngeal airway. C, Relatively small nasopharyngeal airway in the sagittal plane. D, NF type nasopharyngeal airway.
Reference
-
1. Dunn GF, Green LJ, Cunat JJ. Relationships between variation of mandibular morphology and variation of nasopharyngeal airway size in monozygotic twins. Angle Orthod. 1973; 43:129–135.2. Linder-Aronson S. Adenoids. Their effect on mode of breathing and nasal airflow and their relationship to characteristics of the facial skeleton and the denition. A biometric, rhino-manometric and cephalometro-radiographic study on children with and without adenoids. Acta Otolaryngol Suppl. 1970; 265:1–132.3. Subtelny JD, Baker HK. The significance of adenoid tissue in velopharyngeal function. Plast Reconstr Surg (1946). 1956; 17:235–250.
Article4. Caylakli F, Hizal E, Yilmaz I, Yilmazer C. Correlation between adenoid-nasopharynx ratio and endoscopic examination of adenoid hypertrophy: a blind, prospective clinical study. Int J Pediatr Otorhinolaryngol. 2009; 73:1532–1535.
Article5. Selkin SG. Flexible fiberoptics and pediatric otolaryngology. A simple technique for examination and photodocumentation. Int J Pediatr Otorhinolaryngol. 1983; 5:325–333.
Article6. Li AM, Wong E, Kew J, Hui S, Fok TF. Use of tonsil size in the evaluation of obstructive sleep apnoea. Arch Dis Child. 2002; 87:156–159.
Article7. Paradise JL, Bernard BS, Colborn DK, Janosky JE. Assessment of adenoidal obstruction in children: clinical signs versus roentgenographic findings. Pediatrics. 1998; 101:979–986.
Article8. Lertsburapa K, Schroeder JW Jr, Sullivan C. Assessment of adenoid size: A comparison of lateral radiographic measurements, radiologist assessment, and nasal endoscopy. Int J Pediatr Otorhinolaryngol. 2010; 74:1281–1285.
Article9. Aboudara C, Nielsen I, Huang JC, Maki K, Miller AJ, Hatcher D. Comparison of airway space with conventional lateral headfilms and 3-dimensional reconstruction from cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2009; 135:468–479.
Article10. Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am. 2008; 52:707–730.
Article11. Kolo ES, Ahmed AO, Kazeem MJ, Nwaorgu OG. Plain radiographic evaluation of children with obstructive adenoids. Eur J Radiol. 2011; 79:e38–e41.
Article12. Orji FT, Ezeanolue BC. Evaluation of adenoidal obstruction in children: clinical symptoms compared with roentgenographic assessment. J Laryngol Otol. 2008; 122:1201–1205.
Article13. Ogawa T, Enciso R, Shintaku WH, Clark GT. Evaluation of cross-section airway configuration of obstructive sleep apnea. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:102–108.
Article14. Qu X, Li G, Zhang Z, Ma X. Thyroid shields for radiation dose reduction during cone beam computed tomography scanning for different oral and maxillofacial regions. Eur J Radiol. 2012; 81:e376–e380.
Article15. Iwasaki T, Hayasaki H, Takemoto Y, Kanomi R, Yamasaki Y. Oropharyngeal airway in children with Class III malocclusion evaluated by cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2009; 136:318.
Article16. Kim YJ, Hong JS, Hwang YI, Park YH. Three-dimensional analysis of pharyngeal airway in preadolescent children with different anteroposterior skeletal patterns. Am J Orthod Dentofacial Orthop. 2010; 137:306.
Article17. Solow B, Sandham A. Cranio-cervical posture: a factor in the development and function of the dentofacial structures. Eur J Orthod. 2002; 24:447–456.
Article18. Oh KM, Hong JS, Kim YJ, Cevidanes LS, Park YH. Three-dimensional analysis of pharyngeal airway form in children with anteroposterior facial patterns. Angle Orthod. 2011; 81:1075–1082.
Article19. Bartolomé Benito M, Hernández-Sampelayo Matos MT. A radiological assessment of the nasopharynx in healthy children from the Madrid area. An Esp Pediatr. 1998; 49:571–576.20. Brodsky L, Moore L, Stanievich JF. A comparison of tonsillar size and oropharyngeal dimensions in children with obstructive adenotonsillar hypertrophy. Int J Pediatr Otorhinolaryngol. 1987; 13:149–156.
Article21. Hibbert J, Stell PM. A radiological study of the adenoid in normal children. Clin Otolaryngol Allied Sci. 1979; 4:321–327.
Article22. Tagaya M, Nakata S, Yasuma F, Miyazaki S, Sasaki F, Morinaga M, et al. Relationship between adenoid size and severity of obstructive sleep apnea in preschool children. Int J Pediatr Otorhinolaryngol. 2012; 76:1827–1830.
Article23. Marcus CL. Pathophysiology of childhood obstructive sleep apnea: current concepts. Respir Physiol. 2000; 119:143–154.
Article24. Schendel SA, Hatcher D. Automated 3-dimensional airway analysis from cone-beam computed tomography data. J Oral Maxillofac Surg. 2010; 68:696–701.
Article25. Bitar MA, Macari AT, Ghafari JG. Correspondence between subjective and linear measurements of the palatal airway on lateral cephalometric radiographs. Arch Otolaryngol Head Neck Surg. 2010; 136:43–47.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of nasopharyngeal airway and adenoid by MRI
- A longitudinal study of nasopharynx and adenoid growth of Korean children
- Semi-longitudinal study of adenoid and jaw growth of normal occlusal children aged 6 to 17
- The Effects of Adenoidectomy on Nasal Airway Resistance and Nasal Geometry
- Inverse Relationship between Adenoid Size and Asthma or Atopy in Children: A Preliminary Study
