Kinematic Changes in Swallowing After Surgical Removal of Anterior Cervical Osteophyte Causing Dysphagia: A Case Series
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul, Korea. keepwiz@gmail.com
- 2Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2267101
- DOI: http://doi.org/10.5535/arm.2014.38.6.865
Abstract
- This retrospective case series included five patients who underwent surgical resection of the cervical anterior osteophyte due to dysphagia. Videofluoroscopic swallowing studies (VFSSs) were performed before and after surgery on each patient, and kinematic analysis of the video clips from the VFSS of a 5-mL liquid barium swallow was carried out. Functional oral intake improved after surgery in 3/4 patients who had required a modified diet before surgery. Kinematic analysis showed increases in the maximal hyoid vertical movement length (13.16+/-5.87 to 19.09+/-4.77 mm, p=0.080), hyoid movement velocities (170.24+/-84.71 to 285.53+/-104.55 mm/s, p=0.043), and upper esophageal sphincter opening width (3.97+/-0.42 to 6.39+/-1.32 mm, p=0.043) after surgery. In conclusion, improved upper esophageal sphincter opening via enhancement of hyoid movement after cervical anterior osteophyte resection may be the kinetic mechanism of improved swallowing function.
Keyword
MeSH Terms
Figure
-

Fig. 1 Lateral view X-ray (left), preoperative CT (middle), and postoperative CT (right) images of cases. White lines indicate the section level of the CT image, which represents the thickest osteophyte. The level of the thickest osteophyte was C4-5 in 1 case (A) and C5-6 in 4 cases (B-E). CT, computed tomography; VB, vertebral body; OP, osteophyte.
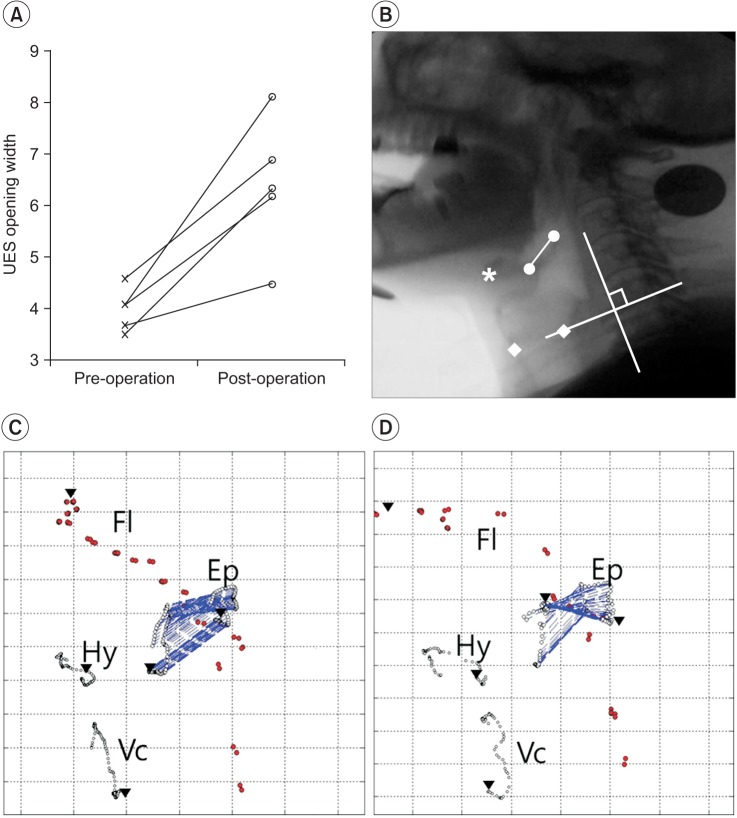
Fig. 2 Exemplary trajectories of the epiglottis. (A) The changes of UES opening width. (B) Cervical lateral view x-ray with digital coordination (•, epiglottis margin; *, anterior margin of hyoid bone; ▪, vocal fold margin; y-axis, a straight line connecting the anterior-inferior border of the 4th cervical vertebra (the '0' point)). (C) Preoperative trajectory. (D) Postoperative trajectory. UES, upper esophageal sphincter; Fl, fluid; Ep, epiglottis; Hy, hyoid; Vc, vocal fold.
Cited by 1 articles
-
Characteristics and Clinical Course of Dysphagia Caused by Anterior Cervical Osteophyte
Hee Eun Choi, Geun Yeol Jo, Woo Jin Kim, Hwan Kwon Do, Jun Koo Kwon, Se Heum Park
Ann Rehabil Med. 2019;43(1):27-37. doi: 10.5535/arm.2019.43.1.27.
Reference
-
1. Carlson ML, Archibald DJ, Graner DE, Kasperbauer JL. Surgical management of dysphagia and airway obstruction in patients with prominent ventral cervical osteophytes. Dysphagia. 2011; 26:34–40. PMID: 20099000.
Article2. Lecerf P, Malard O. How to diagnose and treat symptomatic anterior cervical osteophytes? Eur Ann Otorhinolaryngol Head Neck Dis. 2010; 127:111–116. PMID: 20826123.
Article3. Miyamoto K, Sugiyama S, Hosoe H, Iinuma N, Suzuki Y, Shimizu K. Postsurgical recurrence of osteophytes causing dysphagia in patients with diffuse idiopathic skeletal hyperostosis. Eur Spine J. 2009; 18:1652–1658. PMID: 19714374.
Article4. Song J, Mizuno J, Nakagawa H. Clinical and radiological analysis of ossification of the anterior longitudinal ligament causing dysphagia and hoarseness. Neurosurgery. 2006; 58:913–919. PMID: 16639326.
Article5. Kim DH, Choi KH, Kim HM, Koo JH, Kim BR, Kim TW, et al. Inter-rater reliability of videofluoroscopic dysphagia scale. Ann Rehabil Med. 2012; 36:791–796. PMID: 23342311.
Article6. Paik NJ, Kim SJ, Lee HJ, Jeon JY, Lim JY, Han TR. Movement of the hyoid bone and the epiglottis during swallowing in patients with dysphagia from different etiologies. J Electromyogr Kinesiol. 2008; 18:329–335. PMID: 17187991.
Article7. Angelos C, Dimitra A. Dysphagia due to anterior cervical osteophytes complicated with hypopharynx abscess. BMJ Case Rep. 2011; 2. 23. [Epub]. http://dx.doi.org/10.1136/bcr.11.2010.3551.
Article8. Bilbao G, Duart M, Aurrecoechea JJ, Pomposo I, Igartua A, Catalan G, et al. Surgical results and complications in a series of 71 consecutive cervical spondylotic corpectomies. Acta Neurochir (Wien). 2010; 152:1155–1163. PMID: 20443029.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dysphagia Caused by an Anterior Cervical Osteophyte: A Case Report
- Temporarily Aggravated Dysphagia Following Osteophytectomy and Fixation in a Patient with Cervical Osteophyte
- Giant Anterior Cervical Osteophyte Leading to Dysphagia
- Surgical Treatments on Patients with Anterior Cervical Hyperostosis-Derived Dysphagia
- Characteristics and Clinical Course of Dysphagia Caused by Anterior Cervical Osteophyte
