Ann Rehabil Med.
2012 Aug;36(4):538-543. 10.5535/arm.2012.36.4.538.
The Correlation between Modified Ashworth Scale and Biceps T-reflex and Inter-rater and Intra-rater Reliability of Biceps T-reflex
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University School of Medicine, Yangsan 626-770, Korea. rmshin01@gmail.com
- KMID: 2266725
- DOI: http://doi.org/10.5535/arm.2012.36.4.538
Abstract
OBJECTIVE
To establish a correlation between the modified Ashworth scale (MAS) and amplitude and latency of T-reflex and to demonstrate inter-rater and intra-rater reliability of the T-reflex of the biceps muscle for assessing spasticity after stroke. METHOD: A total of 21 patients with hemiplegia and spasticity after ischemic stroke were enrolled for this study. The spasticity of biceps muscle was evaluated by an occupational therapist using the MAS. The mean value of manual muscle test of biceps muscles was 2.3+/-0.79. Latency and amplitude of T-reflex were recorded from biceps muscles by two physicians. The onset latency and peak to peak amplitude of the mean of 5 big T-reflex were measured. The examinations were carried out by two physicians at the same time to evaluate the inter-rater reliability. Further, one of the physicians performed the examination again after one week to evaluate the intra-rater reliability. The correlations between MAS and T-reflex, and the intra- and inter-rater reliability of biceps T-reflex were established by calculating the Spearman correlation coefficients and the intra-class correlation coefficients (ICCs).
RESULTS
Amplitude of the biceps T-reflex increased with increasing level of MAS (rs=0.464 and 0.573, respectively, p<0.01). ICCs of latency and amplitude of biceps T-reflex were 0.914 and 0.822. The Spearman correlation coefficients of latency and amplitude of biceps T-reflex were 0.937 and 0.635, respectively (p<0.01).
CONCLUSION
Biceps T-reflex demonstrates a good quantitative measurement and correlation tool with MAS for spasticity, and also shows acceptable inter- and intra-rater reliability, which can be used for patients with spasticity after stroke.
Keyword
Figure
-

Fig. 1 Biceps T-reflex tests were performed using a hand operated electric reflex hammer in the relaxed supine position on the affected side.
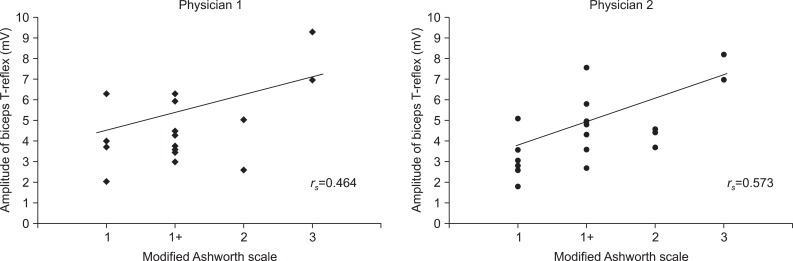
Fig. 2 Correlation between MAS and amplitude of biceps T-reflex; amplitude of biceps T-reflex increased with increasing level of MAS (rs=0.464 and 0.573, respectively, p<0.01).
Reference
-
1. Lance JW, Burke D. Mechanisms of spasticity. Arch Phys Med Rehabil. 1974; 55:332–337. PMID: 4368901.2. Katz RT, Rymer WZ. Spastic hypertonia: mechanisms and measurement. Arch Phys Med Rehabil. 1989; 70:144–155. PMID: 2644919.3. Dimitrijevic MR, Sherwood AM. Spasticity: medical and surgical treatment. Neurology. 1980; 30:19–27. PMID: 6993992.
Article4. Ashby P, Verrier M. Neurophysiologic changes in hemiplegia. Possible explanation for the initial disparity between muscle tone and tendon reflexes. Neurology. 1976; 26:1145–1151. PMID: 1033482.
Article5. Berardelli A, Sabra AF, Hallett M, Berenberg W, Simon SR. Stretch reflexes of triceps surae in patients with upper motor neuron syndromes. J Neurol Neurosurg Psychiatry. 1983; 46:54–60. PMID: 6842201.
Article6. Ashworth B. Preliminary trial of carisoprodol in multiple sclerosis. Practitioner. 1964; 192:540–542. PMID: 14143329.7. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987; 67:206–207. PMID: 3809245.
Article8. Allison SC, Abraham LD, Petersen CL. Reliability of the Modified Ashworth Scale in the assessment of plantarflexor muscle spasticity in patients with traumatic brain injury. Int J Rehabil Res. 1996; 19:67–78. PMID: 8730545.
Article9. Kim CP, Kim SY, Lee JB, Kang BG, Lee YG. Normal values of tendon reflexes in normal Korean adults. J Korean Acad Rehabil Med. 1997; 21:310–316.10. Chon JS, Park CI, Kim SW, Kang JK, Park JH. Quantitative analysis of tendon reflexes in Korean normal adults. J Korean Acad Rehabil Med. 1996; 20:741–747.11. Yoon TS, Kim JA. Quantitative analysis of tendon reflexes of upper extremities in normal volunteers. J Korean Acad Rehabil Med. 1999; 23:310–315.12. Frijns CJ, Laman DM, van Duijn MA, van Duijn H. Normal values of patellar and ankle tendon reflex latencies. Clin Neurol Neurosurg. 1997; 99:31–36. PMID: 9107465.
Article13. Schott K, Koeniq E. T-wave response in cervical root lesions. Acta Neurol Scand. 1991; 84:273–276. PMID: 1771998.
Article14. Gregson JM, Leathley M, Moore AP, Sharma AK, Smith TL, Watkins CL. Reliability of the Tone Assessment Scale and the modified Ashworth scale as clinical tools for assessing poststroke spasticity. Arch Phys Med Rehabil. 1999; 80:1013–1016. PMID: 10489001.
Article15. Karam DB. Tendon reflex latencies in the upper extremity. Arch Phys Med Rehabil. 1977; 58:306–308. PMID: 195557.16. Kuruoglu HR, Oh SJ. Tendon-reflex testing in chronic demyelinating polyneuropathy. Muscle Nerve. 1994; 17:145–150. PMID: 8114782.
Article17. Kuruoglu R, Oh SJ. Quantitation of tendon reflexes in normal volunteers. Electromyogr Clin Neurophysiol. 1993; 33:347–351. PMID: 8223334.18. Kim HD, Park IS, Song YJ. Comparison of tendon reflex responses between two heads of gastrocnemius in spastic hemiplegia and healthy subjects. J Korean Acad Rehabil Med. 1998; 22:1173–1178.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intra and Inter-Rater Measurement Reliability of Tibialis Anterior Muscle (TA) Thickness using the Ultrasonography Spring Gauge Technique
- The Validity and Reliability of the EMC Device; For the Checking ofthe Mobility of the First Ray of the Foot
- Reliability of Hip Migration Index in Children with Cerebral Palsy: The Classic and Modified Methods
- Extraction of the pull force from inertial sensors during the pull test for Parkinson’s disease: A reliability study
- The reliability of an easy measuring method for abutment convergence angle with a computer-aided design (CAD) system
