Management of Severe Bilateral Ptosis in a Patient With Midbrain Infarction: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, St. Paul's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. coltrane@catholic.ac.kr
- KMID: 2266570
- DOI: http://doi.org/10.5535/arm.2013.37.6.891
Abstract
- Ptosis could be caused by oculomotor nerve palsy in the midbrain infarction. Bilateral ptosis has been reported in several reports, which focused on clinical characteristics of midbrain infarction. Little research attention has been paid to the treatment of patients with bilateral ptosis in midbrain infarction. We experienced a case of severe bilateral ptosis occurring after midbrain infarction. The patient could not open her eyes, perform basic activities or achieve effective rehabilitation. Neurogenic ptosis can improved after the underlying cause is treated. However, in this case, bilateral ptosis was not improved after conservative care for 6 months and the patient remained limited in activities of daily living and mobility. Surgical correction of bilateral ptosis was done by the resection of both Muller's muscles. After surgical correction, the bilateral ptosis was much improved and the effect persisted for at least 6 months.
MeSH Terms
Figure
-
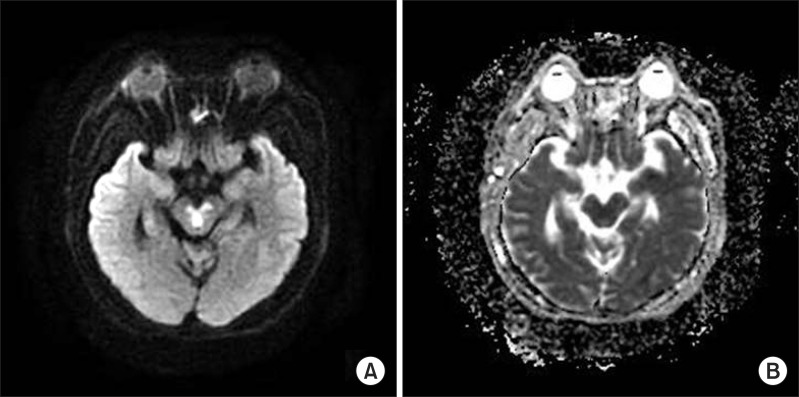
Fig. 1 Brain diffusion-weighted imaging and apparent diffusion coefficient map at clinical onset. (A) Axial diffusion-weighted imaging demonstrates increased signal in the bilateral paramedian midbrain. (B) Apparent diffusion coefficient map demonstrates hypointense signal in corresponding areas, consistent with restricted diffusion.

Fig. 2 Follow-up photographs of the patient's eyelids. (A) Before surgery, the patient had complete bilateral ptosis. Ptosis was 7 mm and the levator function was 0 mm on both eyes. The palpebral fissure height was uncheckable. (B) We tried to tape the eyelids using Micropore tape. However, this method was less efficient due to the blinking mechanism. (C) After surgery, the ptosis was improved by 4 mm on the right side and 4.5 mm on the left side. The palpebral fissure height was 3.5 mm on the right side and 3.0 mm on the left side.
Reference
-
1. Kim JS, Kim J. Pure midbrain infarction: clinical, radiologic, and pathophysiologic findings. Neurology. 2005; 64:1227–1232. PMID: 15824351.
Article2. Bogousslavsky J, Maeder P, Regli F, Meuli R. Pure midbrain infarction: clinical syndromes, MRI, and etiologic patterns. Neurology. 1994; 44:2032–2040. PMID: 7969955.3. Ogawa K, Suzuki Y, Oishi M, Kamei S. Clinical study of twenty-one patients with pure midbrain infarction. Eur Neurol. 2012; 67:81–89. PMID: 22189277.
Article4. Thurtell MJ, Halmagyi GM. Complete ophthalmoplegia: an unusual sign of bilateral paramedian midbrain-thalamic infarction. Stroke. 2008; 39:1355–1357. PMID: 18309144.5. Donzelli R, Marinkovic S, Brigante L, Nikodijevic I, Maiuri F, de Divitiis O. The oculomotor nuclear complex in humans: microanatomy and clinical significance. Surg Radiol Anat. 1998; 20:7–12. PMID: 9574483.
Article6. Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. 2003; 27:193–204. PMID: 12925861.
Article7. Betharia SM, Kalra BR. Observations on Bell's phenomenon after levator surgery. Indian J Ophthalmol. 1985; 33:109–111. PMID: 3833733.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Elastic Eyelid Band Application on Bilateral Severe Ptosis in a Patient With Bilateral Incomplete Claude’s Syndrome: A Case Report
- A Case of Bilateral Oculomotor Nuclear Palsy
- Four Cases of Paramedian Thalamopeduncular Artery Infarction
- A Case of Midbrain Hemorrhage Presenting as Bilateral Ptosis with Diurnal Fluctuation
- Roles of Diagnostic Cerebral Angiography and High-resolution Vessel-wall Imaging in Evaluating Basilar Artery Perforators: A Case of Bilateral Midbrain Infarction
