Allergy Asthma Respir Dis.
2013 Sep;1(3):288-291. 10.4168/aard.2013.1.3.288.
Kartagener's syndrome with immunoglobulin G subclass deficiency
- Affiliations
-
- 1Department of Allergy & Clinical Immunology, Ajou University School of Medicine, Suwon, Korea. ye9007@ajou.ac.kr
- KMID: 2262974
- DOI: http://doi.org/10.4168/aard.2013.1.3.288
Abstract
- Kartagener syndrome is characterized by the triad of situs inversus, bronchiectasis, and chronic paranasal sinusitis. Recurrent sinopulmonary infection, the major determinant for diagnosing immunodeficiency, is the most common clinical manifestation of the disease. A 17-year-old female patient presented with dyspnea, cough, sputum, nasal congestion, and rhinorrhea for more than 5 years. Nasal symptoms and dyspnea had not been controlled by intermittent treatment with mucolytics and antibiotics from primary clinics since 3 months before visiting our clinic. Chest X-ray and computed tomography showed situs inversus, dextrocardia and bronchiectasis. Paranasal sinus series revealed mucosal thickening and haziness on both maxillary sinus. Serum immunoglobulin (Ig) G4 was decreased, but total IgG was within normal range. Under the diagnosis of Kartagener syndrome with IgG4 deficiency, monthly intravenous IgG (IVIG) treatment was performed for 6 months. Her symptoms were well controlled and the frequency of antibiotics use was markedly decreased. We report a patient having the Kartagener syndrome with IgG4 deficiency that was successfully controlled with a 6-month-treatment of IVIG.
MeSH Terms
-
Adolescent
Anti-Bacterial Agents
Bronchiectasis
Cough
Dextrocardia
Dyspnea
Estrogens, Conjugated (USP)
Expectorants
Female
Humans
Immunoglobulin G
Immunoglobulins
Immunoglobulins, Intravenous
Kartagener Syndrome
Maxillary Sinus
Reference Values
Sinusitis
Situs Inversus
Sputum
Thorax
Anti-Bacterial Agents
Estrogens, Conjugated (USP)
Expectorants
Immunoglobulin G
Immunoglobulins
Immunoglobulins, Intravenous
Figure
-
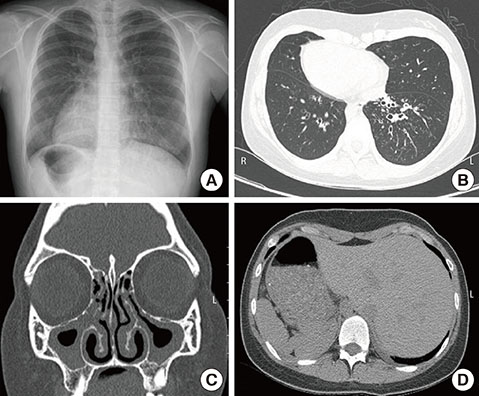
Fig. 1 Radiologic findings at the time of diagnosis. (A) Chest X-ray shows situs inversus with dextrocardia. (B) Chest computerized tomography (CT) shows dextrocardia and bronchiectasis with mucoid impaction in both lower lobes. (C) Paranasal sinus CT shows prominent and diffuse mucoperiosteal thickening on entire paranasal sinus. (D) Abdominal CT shows a mirror image of normal configuration of stomach and liver.

Fig. 2 Ultrastructural findings of cilia of nasal mucosa show partial defect of outer (→) and inner (-->) dynein arm.
Cited by 1 articles
-
Three Cases of IgG4-Related Sclerosing Disease in Nasal Cavity
Jae Ryung Lee, Bong-Jae Lee, Yoo-Sam Chung
J Rhinol. 2016;23(1):44-48. doi: 10.18787/jr.2016.23.1.44.
Reference
-
1. Fishman AP, Elias JA, Fishman JA, Grippi MA, Kaiser LR, Senior RM. Fishman's pulmonary diseases and disorders. New York: McGraw-Hill Inc;1997.2. Afzelius BA, Stenram U. Prevalence and genetics of immotile-cilia syndrome and left-handedness. Int J Dev Biol. 2006; 50:571–573.
Article3. Skorpinski EW, Kung SJ, Yousef E, McGeady SJ. Diagnosis of common variable immunodeficiency in a patient with primary ciliary dyskinesia. Pediatrics. 2007; 119:e1203–e1205.
Article4. Smith DW. Recognisable patterns of human malformation. 3rd ed. Philadelphia: WB Saunders;1982.5. Hogg C. Primary ciliary dyskinesia: when to suspect the diagnosis and how to confirm it. Paediatr Respir Rev. 2009; 10:44–50.
Article6. Eliasson R, Mossberg B, Camner P, Afzelius BA. The immotile-cilia syndrome: a congenital ciliary abnormality as an etiologic factor in chronic airway infections and male sterility. N Engl J Med. 1977; 297:1–6.7. Afzelius BA. A human syndrome caused by immotile cilia. Science. 1976; 23. 193:317–319.
Article8. Sturgess JM, Chao J, Wong J, Aspin N, Turner JA. Cilia with defective radial spokes: a cause of human respiratory disease. N Engl J Med. 1979; 300:53–56.9. Lie H, Ferkol T. Primary ciliary dyskinesia: recent advances in pathogenesis, diagnosis and treatment. Drugs. 2007; 67:1883–1892.10. Yang SC, Lee KS, Yoon HJ, Shin DH, Park SS, Lee JH, et al. A case of Kartagener's syndrome presenting as respiratory and right heart failure. Tuberc Respir Dis. 1996; 43:251–256.
Article11. Paeck KH, Lee KY, Min KH, Park SJ, Lee HB, Lee YC, et al. A case of Kartagener's syndrome with acute respiratory failure successfully treated by NPPV. Korean J Med. 2007; 73:976–980.12. Moss RB, Carmack MA, Esrig S. Deficiency of IgG4 in children: association of isolated IgG4 deficiency with recurrent respiratory tract infection. J Pediatr. 1992; 120:16–21.
Article13. Heiner DC. IgG4 immunodeficiency. N Engl Reg Allergy Proc. 1988; 9:43–50.
Article14. Orange JS, Hossny EM, Weiler CR, Ballow M, Berger M, Bonilla FA, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol. 2006; 117:4 Suppl. S525–S553.
Article15. Abdou NI, Greenwell CA, Mehta R, Narra M, Hester JD, Halsey JF. Efficacy of intravenous gammaglobulin for immunoglobulin G subclass and/or antibody deficiency in adults. Int Arch Allergy Immunol. 2009; 149:267–274.
Article16. Jefferis R, Kumararatne DS. Selective IgG subclass deficiency: quantification and clinical relevance. Clin Exp Immunol. 1990; 81:357–367.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Chronic Intractable Diarrhea with IgA, IgG2 and IgG4 Deficiency
- A case of intravenous immunoglobulin therapy in severe aspirin - sensitive asthma patient combined with IgG1 and IgG3 subclass deficiency
- A case of a patient with IgG3 subclass deficiency and recurrent fungal infection of oral cavity
- Two Cases of Malignant Lymphomas in Children with Selective IgA and IgG Subclass Deficiency
- Diagnosis and treatment of immunoglobulin G subclass deficiency in a school-age child with recurrent wheezing
