Critical pathway of acute asthma attack for the Emergency Center: patients' outcomes and effectiveness
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. PARKJW@yuhs.ac
- 2Institute of Allergy, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2262273
- DOI: http://doi.org/10.4168/aard.2015.3.1.30
Abstract
- PURPOSE
Early recognition and management of asthma attack is critical before it becomes worse. We developed critical pathway (CP) of asthma attack at Emergency Center (EC) for making undelayed decision and management of asthma attack.
METHODS
Acute asthma attack assessment and treatment (4AT) CP began on April 1st 2012 and recruited the patients for 18 months. This study enrolled the patients who were older than 15 years and visited EC for dyspnea and wheezing. Initial assessment was done measuring peak expiratory flow rate (PEFR), oxygen saturation (SaO2). Once CP is activated, oxygen, inhalation of short acting beta2 agonist, and injection of corticosteroid were administered to the patients. Every hour after CP activated, we reassess the patients' response and make decisions whether to admit or discharge.
RESULTS
Until January 10th 2014, 62 patients enrolled in this study. Seven patients hospitalized for asthma and 40 patients discharged. The other 15 patients were deactivated as they were diagnosed of heart failure, myocardial infarction, aortic dissection, anaphylaxis, chronic obstructive pulmonary disease and pneumonia for the causes of dyspnea. Mean Interval from EC arrival to 4AT activation was 32.6+/-29.1 minutes and the mean interval from 4AT activation to position decision was 254.5+/-302.0 minutes. Among 47 patients who were diagnosed with asthma attack, 13 patients were not aware of asthma before this attack. Forty patients were discharged at EC after management of CP. Among them, 34 patients revisited clinic, but 6 patients did not. We called back to the lost 6 patients but only 3 patients were connected. Even they visited EC due to asthma attack, 2 patients had no insight of importance of regular management and the other one promised to revisit.
CONCLUSION
CP was successful for early management of asthma attack. However, 15% of discharged patients never show up again. So, education program about the importance of ongoing management of asthma for prevention of asthma attack is needed.
Keyword
MeSH Terms
Figure
-

Fig. 1. Acute asthma attack assessment and treatment critical pathway (CP) flow of this study. Included patients are who visits emergency center (EC) for dyspnea and wheezing. Patients who had dyspnea and wheezing caused by cardiovascular diseases, other pulmonary diseases or malignancy rather than asthma were excluded. After initial treatments, patients were reassessed their response every hour by measured peak expiratory flow rate (PEFR) and SaO2. Responsiveness assessed 3 categories. Favorable response was patients who were resolved wheezing sound and dyspnea, increased PEFR more than 150% from basal measurement and SaO2 checked more than 92%. Incomplete response was patients who were remaining wheezing and dyspnea, didn't ex-ceed SaO2 more than 92%, and increased PEFR less than 150% from basal. Poor response include patients who were increased PEFR less than 30% from basal, PaO2 less than 60 mmHg and/or PaCO2 more than 45 mmHg in arterial blood gas analysis. When reassessment proceed, made a decision either admission or discharge. P/Ex, physical examination; EKG, electrocardiography; MI, myocardial infarction; UA, unstable angina; CHF, congestive heart failure; IV, in-travenous; SaO2, arterial oxygen saturation; PaCO2, partial pressure of arterial carbon dioxide; PaO2, partial pressure of arterial oxygen; min, minutes; ICU, intensive care uint; PRN, pro re nata; Mcg, microgram; BID, bis in die.
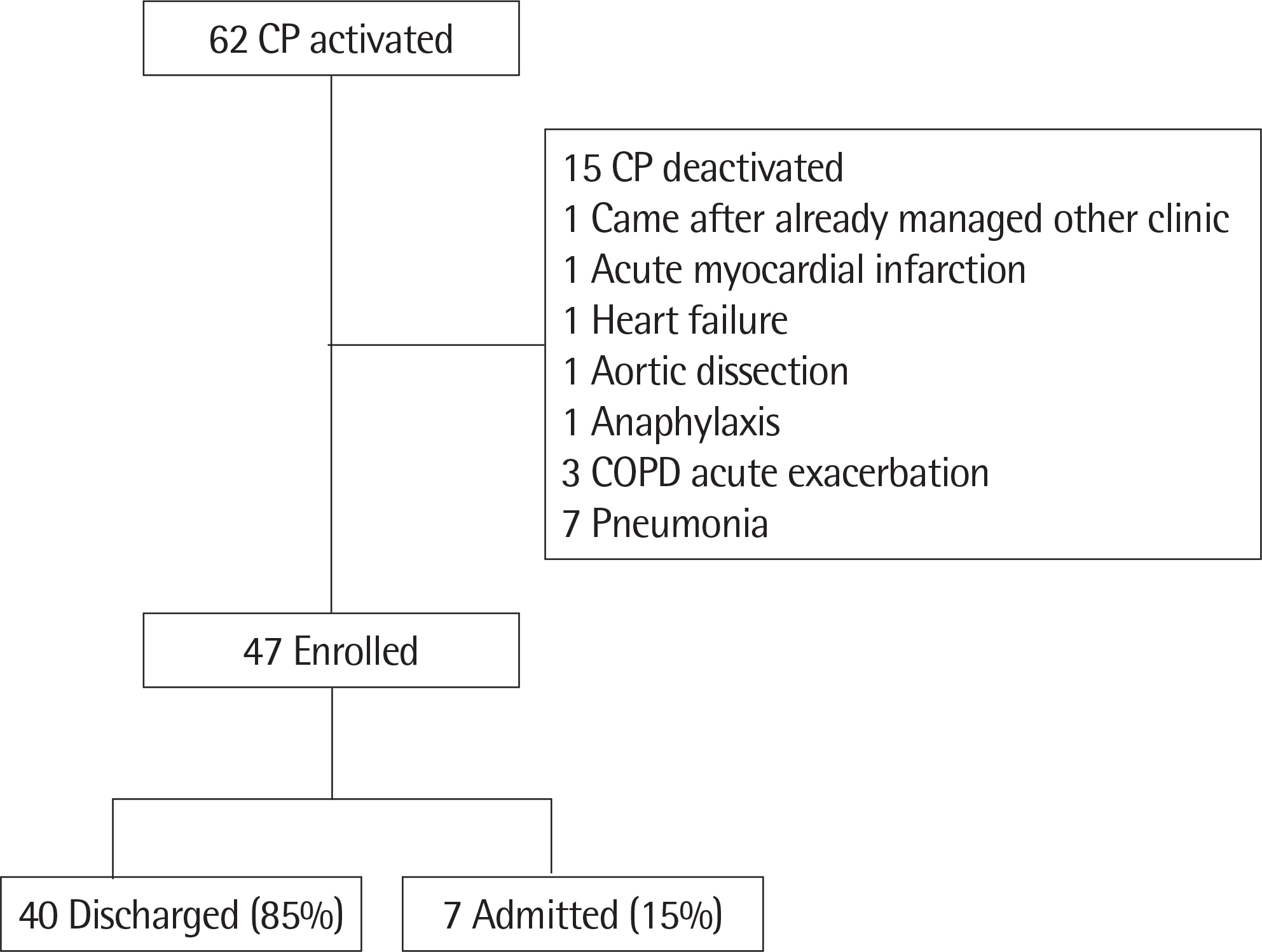
Fig. 2. Patients flow of this study. Total 62 patients were enrolled in 4AT (acute asthma attack assessment and treatment) CP program. Fifteen patients were diagnosed as other disease for their cause of dyspnea and deactivated. Along finally enrolled 47 patients, 40 patients (85%) discharged, and 7 patients (15%) admitted. CP, critical pathway; COPD, chronic obstructive pulmonary disease.
Reference
-
References
1. The Global Initiative for Asthma. GINA Report, Global strategy for asthma management and prevention. Revised 2014 [Internet]. The Global Initiative for Asthma;c2014. [cited 2014 Jun 11]. Available from:. http://www.ginasthma.org/local/uploads/files/GINA_Report_2014_Jun11.pdf.2. Ministry of Health & Welfare; Korea Centers for Disease Control and Prevention. Korea Health Statistics 2012: Korea National Health and Nutrition Examination Survey (KNHANES V-3). Cheongwon: Ministry of Health & Welfare, Korea Centers for Disease Control and Prevention;2013.3. Sullivan SD, Weiss KB. Health economics of asthma and rhinitis. II. Assessing the value of interventions. J Allergy Clin Immunol. 2001; 107:203–10.
Article4. Weiss KB, Sullivan SD, Lyttle CS. Trends in the cost of illness for asthma in the United States, 1985–1994. J Allergy Clin Immunol. 2000; 106:493–9.
Article5. Weiss KB, Sullivan SD. The health economics of asthma and rhinitis. I. Assessing the economic impact. J Allergy Clin Immunol. 2001; 107:3–8.
Article6. Hoskins G, McCowan C, Neville RG, Thomas GE, Smith B, Silverman S. Risk factors and costs associated with an asthma attack. Thorax. 2000; 55:19–24.
Article7. Dy SM, Garg P, Nyberg D, Dawson PB, Pronovost PJ, Morlock L, et al. Critical pathway effectiveness: assessing the impact of patient, hospital care, and pathway characteristics using qualitative comparative analysis. Health Serv Res. 2005; 40:499–516.
Article8. Bailey R, Weingarten S, Lewis M, Mohsenifar Z. Impact of clinical pathways and practice guidelines on the management of acute exacerbations of bronchial asthma. Chest. 1998; 113:28–33.
Article9. Berenholtz S, Pronovost P, Lipsett P, Dawson P, Dorman T. Assessing the effectiveness of critical pathways on reducing resource utilization in the surgical intensive care unit. Intensive Care Med. 2001; 27:1029–36.
Article10. Gadacz TR, Adkins RB Jr, O'Leary JP. General surgical clinical pathways: an introduction. Am Surg. 1997; 63:107–10.11. Weiland DE. Why use clinical pathways rather than practice guidelines? Am J Surg. 1997; 174:592–5.
Article12. Wazeka A, Valacer DJ, Cooper M, Caplan DW, DiMaio M. Impact of a pediatric asthma clinical pathway on hospital cost and length of stay. Pediatr Pulmonol. 2001; 32:211–6.
Article13. Norton SP, Pusic MV, Taha F, Heathcote S, Carleton BC. Effect of a clinical pathway on the hospitalisation rates of children with asthma: a prospective study. Arch Dis Child. 2007; 92:60–6.
Article14. Burgers PT, Van Lieshout EM, Verhelst J, Dawson I, de Rijcke PA. Implementing a clinical pathway for hip fractures; effects on hospital length of stay and complication rates in five hundred and twenty six patients. International orthopaedics. 2014; 38:1045–50.
Article15. Goldberg R, Chan L, Haley P, Harmata-Booth J, Bass G. Critical pathway for the emergency department management of acute asthma: effect on resource utilization. Ann Emerg Med. 1998; 31:562–7.
Article16. Lazarus SC. Clinical practice. Emergency treatment of asthma. N Engl J Med. 2010; 363:755–64.17. Moorman JE, Akinbami LJ, Bailey CM. National Surveillance of Asthma: United States, 2001–2010. National Center for Health Statistics. Vital Health Stat. 2012; 35:1–67.18. Rowe BH, Voaklander DC, Wang D, Senthilselvan A, Klassen TP, Marrie TJ, et al. Asthma presentations by adults to emergency departments in Alberta, Canada: a large population-based study. Chest. 2009; 135:57–65.19. Rowe BH, Bota GW, Clark S, Camargo CA. Multicenter Airway Research Collaboration Investigators. Comparison of Canadian versus American emergency department visits for acute asthma. Can Respir J. 2007; 14:331–7.
Article20. Ray P, Birolleau S, Lefort Y, Becquemin MH, Beigelman C, Isnard R, et al. Acute respiratory failure in the elderly: etiology, emergency diagnosis and prognosis. Crit Care. 2006; 10:R82.21. Malas O, Caglayan B, Fidan A, Ocal Z, Ozdogan S, Torun E. Cardiac or pulmonary dyspnea in patients admitted to the emergency department. Respir Med. 2003; 97:1277–81.
Article22. Manivannan V, Decker WW, Bellolio MF, Stead LG, Li JT, Vedula A, et al. Prescriptions for self-injectable epinephrine in emergency department angioedema management. Ann Allergy Asthma Immunol. 2011; 106:489–93.
Article23. Sampson HA, Munoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: summary report: second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. Ann Emerg Med. 2006; 47:373–80.24. Stein PD, Beemath A, Matta F, Weg JG, Yusen RD, Hales CA, et al. Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am J Med. 2007; 120:871–9.
Article25. The Global Initiative for Asthma. Global Strategy for Diagnosis, Management, and Prevention of COPD. January 2014 [Internet]. The Global Initiative for Asthma;c2011. [cited 2014 May 5]. Available from:. http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html.26. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007; 44(Suppl 2):S27–72.
Article27. Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med. 2000; 342:868–74.
Article28. Glickman SW, Shofer FS, Wu MC, Scholer MJ, Ndubuizu A, Peterson ED, et al. Development and validation of a prioritization rule for obtaining an immediate 12-lead electrocardiogram in the emergency department to identify ST-elevation myocardial infarction. Am Heart J. 2012; 163:372–82.
Article29. Mueller C, Frana B, Rodriguez D, Laule-Kilian K, Perruchoud AP. Emergency diagnosis of congestive heart failure: impact of signs and symptoms. Can J Cardiol. 2005; 21:921–4.30. Ganz LI, Friedman PL. Supraventricular tachycardia. N Engl J Med. 1995; 332:162–73.
Article31. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014; 130:2071–104.
Article32. Bronstein AC, Spyker DA, Cantilena LR Jr, Green JL, Rumack BH, Giffin SL. 2008 Annual Report of the American Association of Poison Control Centers' National Poison Data System (NPDS): 26th Annual Report. Clin Toxicol (Phila). 2009; 47:911–1084.
Article33. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013; 39:165–228.
Article34. Sulter G, Elting JW, Stewart R, den Arend A, De Keyser J. Continuous pulse oximetry in acute hemiparetic stroke. J Neurol Sci. 2000; 179(S 1–2):65–9.
Article35. Bass C. Chest pain and breathlessness: relationship to psychiatric illness. Am J Med. 1992; 92(1A):12S–7S.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Pathway for Childhood Asthma in an Emergency Department: Comparison Between the Correct Versus Incorrect Application Groups
- An analysis on the treatment outcome of acute asthma attack
- Recent Trend in Prevalence and Severity of Acute Asthma in an Emergency Room
- Implementation of a Critical Pathway to the Dizzy Patients in the Emergency Center
- Development of Critical Pathway for Laparoscopic Assisted Vaginal Hysterectomy by CPA program
