Allergy Asthma Immunol Res.
2014 Mar;6(2):169-174. 10.4168/aair.2014.6.2.169.
Reference Values and Determinants of Fractional Concentration of Exhaled Nitric Oxide in Healthy Children
- Affiliations
-
- 1Department of Pediatrics, Childhood Asthma Atopy Center, Asan Medical Center, Ulsan University College of Medicine, Seoul, Korea. sjhong@amc.seoul.kr
- 2Department of Pediatrics, CHA University School of Medicine, Seongnam, Korea.
- 3Research Center for Standardization of Allergic Diseases, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Pediatrics, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea.
- 5Department of Pediatrics, Korea Cancer Center Hospital, Seoul, Korea.
- 6Department of Pediatrics, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 7Department of Pediatrics, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 8Department of Pediatrics, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 9Department of Pediatrics, Hallym Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 10Department of Pediatrics, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea.
- 11Department of Pediatrics, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 12Department of Pediatrics, National Health Insurance Corporation Ilsan Hospital, Seoul, Korea.
- 13Department of Pediatrics, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2260263
- DOI: http://doi.org/10.4168/aair.2014.6.2.169
Abstract
- PURPOSE
Measurement of the fractional concentration of exhaled nitric oxide (FeNO) is a quantitative, noninvasive, simple, safe method of assessing airway inflammation. While FeNO measurement has been standardized, reference values for elementary school children are scarce. The aim of this study was to establish reference values for FeNO in children.
METHODS
FeNO was measured in elementary school children at 6-12 years of age in Seoul, Korea, following American Thoracic Society guidelines and using a chemiluminescence analyzer (NIOX Exhaled Nitric Oxide Monitoring System, Aerocrine, Sweden). A total of 1,252 children completed a modified International Study of Asthma and Allergy in Children (ISAAC) questionnaire; FeNO was measured in 1,063 children according to the protocol and in 808 children defined as healthy controls.
RESULTS
Mean FeNO were 10.32 ppb, 16.58 ppb, and 12.36 ppb in non-atopic, atopic, and all 808 healthy controls, respectively. FeNO was not associated with age and gender. The FeNO reference equations were determined by multiple linear regression analysis, taking into account the variables of age, height, weight, total IgE, eosinophil percent, and bronchial hyper-responsiveness (methacholine PC20). FeNO=0.776 + 0.003 x total IgE + 0.340 x eosinophil percent; coefficient of determination (R2)=0.084 in the 501 healthy non-atopic controls. FeNO=-18.365 + 1.536 x eosinophil percent, R2=0.183 in the 307 healthy atopic controls; and FeNO=-7.888 + 0.130 x Height + 0.004 x total IgE + 1.233 x eosinophil percent, R2=0.209 in the 808 all healthy controls. Eosinophil percent was correlated with FeNO in all healthy controls. FeNO was not associated with BMI.
CONCLUSION
This study provides reference values for FeNO that can be used to evaluate airway inflammation in elementary school children. Determinants that could most accurately predict FeNO in healthy school-age children were assessed.
Keyword
MeSH Terms
Figure
-
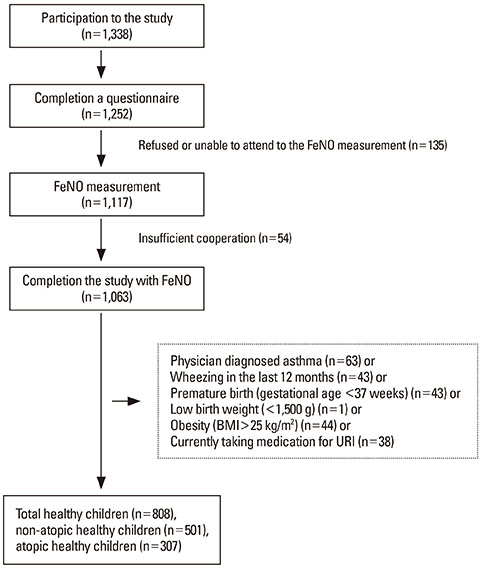
Figure Schematic presentation of the recruitment of healthy children. BMI, body mass index; URI, upper respiratory infection.
Cited by 2 articles
-
Fractional exhaled nitric oxide in Korean children with allergic rhinitis
Seung Hyun Moon, Hae Ji Jang, Yoon Sung Park, Woo Yeon Lee, Dae Hyun Lim, Jeong Hee Kim
Allergy Asthma Respir Dis. 2015;3(6):439-445. doi: 10.4168/aard.2015.3.6.439.The association of forced expiratory volume in one second and forced expiratory flow at 50% of the vital capacity, peak expiratory flow parameters, and blood eosinophil counts in exercise-induced bronchospasm in children with mild asthma
H. Haluk Akar, Fulya Tahan, Hatice Eke Gungor
Asia Pac Allergy. 2015;5(2):98-102. doi: 10.5415/apallergy.2015.5.2.98.
Reference
-
1. Malmberg LP, Petäys T, Haahtela T, Laatikainen T, Jousilahti P, Vartiainen E, Mäkelä MJ. Exhaled nitric oxide in healthy nonatopic school-age children: determinants and height-adjusted reference values. Pediatr Pulmonol. 2006; 41:635–642.2. Buchvald F, Baraldi E, Carraro S, Gaston B, De Jongste J, Pijnenburg MW, Silkoff PE, Bisgaard H. Measurements of exhaled nitric oxide in healthy subjects age 4 to 17 years. J Allergy Clin Immunol. 2005; 115:1130–1136.3. Kwon JW, Kim BJ, Song Y, Seo JH, Kim TH, Yu J, Kim HB, Lee SY, Kim WK, Kim KW, Ji HM, Kim KE, Kim H, Hong SJ. Changes in the prevalence of childhood asthma in Seoul from 1995 to 2008 and its risk factors. Allergy Asthma Immunol Res. 2011; 3:27–33.4. Kim WK, Kwon JW, Seo JH, Kim HY, Yu J, Kim BJ, Kim HB, Lee SY, Kim KW, Kang MJ, Shin YJ, Hong SJ. Interaction between IL13 genotype and environmental factors in the risk for allergic rhinitis in Korean children. J Allergy Clin Immunol. 2012; 130:421–426.e5.5. Lee SY, Kwon JW, Seo JH, Song YH, Kim BJ, Yu J, Park KS, Kim H, Kim EJ, Lee JS, Hong SJ. Prevalence of atopy and allergic diseases in Korean children: associations with a farming environment and rural lifestyle. Int Arch Allergy Immunol. 2012; 158:168–174.6. Standardization of Spirometry, 1994 Update. American Thoracic Society. Am J Respir Crit Care Med. 1995; 152:1107–1136.7. Jörres RA, Nowak D, Kirsten D, Grönke L, Magnussen H. A short protocol for methacholine provocation testing adapted to the Rosenthal-Chai dosimeter technique. Chest. 1997; 111:866–869.8. Kim BJ, Kwon JW, Seo JH, Kim HB, Lee SY, Park KS, Yu J, Kim HC, Leem JH, Sakong J, Kim SY, Lee CG, Kang DM, Ha M, Hong YC, Kwon HJ, Hong SJ. Association of ozone exposure with asthma, allergic rhinitis, and allergic sensitization. Ann Allergy Asthma Immunol. 2011; 107:214–219.e1.9. American Thoracic Society. European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005; 171:912–930.10. Lee JY, Seo JH, Kim HY, Jung YH, Kwon JW, Kim BJ, Kim HB, Lee SY, Jang GC, Song DJ, Kim WK, Shim JY, Kim HJ, Shin YJ, Park JW, Cho SH, Lee JS, Hong SJ. Reference values of impulse oscillometry and its utility in the diagnosis of asthma in young Korean children. J Asthma. 2012; 49:811–816.11. Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, Olin AC, Plummer AL, Taylor DR. American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011; 184:602–615.12. Kovesi T, Kulka R, Dales R. Exhaled nitric oxide concentration is affected by age, height, and race in healthy 9- to 12-year-old children. Chest. 2008; 133:169–175.13. Linn WS, Rappaport EB, Berhane KT, Bastain TM, Avol EL, Gilliland FD. Exhaled nitric oxide in a population-based study of southern California schoolchildren. Respir Res. 2009; 10:28.14. Kharitonov SA, Gonio F, Kelly C, Meah S, Barnes PJ. Reproducibility of exhaled nitric oxide measurements in healthy and asthmatic adults and children. Eur Respir J. 2003; 21:433–438.15. Zhang H, Shu L, Cai X, Wang Z, Jiao X, Liu F, Hou P, Wang L, Shan L, Chen N, Shang Y. Gender and age affect the levels of exhaled nitric oxide in healthy children. Exp Ther Med. 2013; 5:1174–1178.16. Tsang KW, Ip SK, Leung R, Tipoe GL, Chan SL, Shum IH, Ip MS, Yan C, Fung PC, Chan-Yeung M, Lam W. Exhaled nitric oxide: the effects of age, gender and body size. Lung. 2001; 179:83–91.17. Franklin PJ, Taplin R, Stick SM. A community study of exhaled nitric oxide in healthy children. Am J Respir Crit Care Med. 1999; 159:69–73.18. Kim SH, Kim TH, Sohn JW, Yoon HJ, Shin DH, Park SS. Reference values and determinants of exhaled nitric oxide in healthy Korean adults. J Asthma. 2010; 47:563–567.19. Steerenberg PA, Janssen NA, de Meer G, Fischer PH, Nierkens S, van Loveren H, Opperhuizen A, Brunekreef B, van Amsterdam JG. Relationship between exhaled NO, respiratory symptoms, lung function, bronchial hyperresponsiveness, and blood eosinophilia in school children. Thorax. 2003; 58:242–245.20. Baroffio M, Barisione G, Crimi E, Brusasco V. Noninflammatory mechanisms of airway hyper-responsiveness in bronchial asthma: an overview. Ther Adv Respir Dis. 2009; 3:163–174.21. Baraldi E, Azzolin NM, Cracco A, Zacchello F. Reference values of exhaled nitric oxide for healthy children 6-15 years old. Pediatr Pulmonol. 1999; 27:54–58.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Measurements of fractional exhaled nitric oxide in pediatric asthma
- Measurements of Exhaled Nitric Oxide in Newborns
- Utility of Fractional Exhaled Nitric Oxide in the Diagnosis of Asthma and the Assessment of Asthma Control
- Measurement and Interpretation of Fractional Exhaled Nitric Oxide
- Exhaled NO: Determinants and Clinical Application in Children With Allergic Airway Disease
