A Case of Massive Intravascular Hemolysis Associated with Clostiridium perfringens Sepsis
- Affiliations
-
- 1Department of Laboratory Medicine, East-West Neo Medical Center, Kyung Hee University College of Medicine, Seoul, Korea. wileemd@khu.ac.kr
- KMID: 2252228
- DOI: http://doi.org/10.5045/kjh.2007.42.4.409
Abstract
- Clostridium perfringens is an anaerobic, gram-positive rod that inhabits the soil and the intestinal tracts of many animals, including humans. C. perfringens is a major cause of food poisoning, traumatic or nontraumatic myonecrosis, clostridial cellulitis, gangrenous cholecystitis, sepsis or bacteremia, and intravascular hemolysis. Massive intravascular hemolysis is a rare complication of C. perfringens septicemia and has a high mortality rate with an extremely rapid progression. Therefore, aggressive treatment is required as soon as the diagnosis is made. In this study, we report a case of massive intravascular hemolysis due to C. perfringens septicemia in a 34-year-old man with liver cirrhosis.
MeSH Terms
Figure
-

Fig. 1 WBC, RBC, and PLT histograms (Coulter LH750, Beckman Coulter, Inc, CA, USA) showed unusual patterns. Especially most of RBC were small sized. Mean corpuscular volume was 53.9fL (A, B, and C). WBC scattergram showed bad separation of the population; the segmented neutrophil population (pink area) was mixed with monocyte population (green area), and lymphocyte population (blue area). The manual count of white blood cells revealed 63% segmented neutrophils, 25% lymphocytes, and 12% monocytes (D).
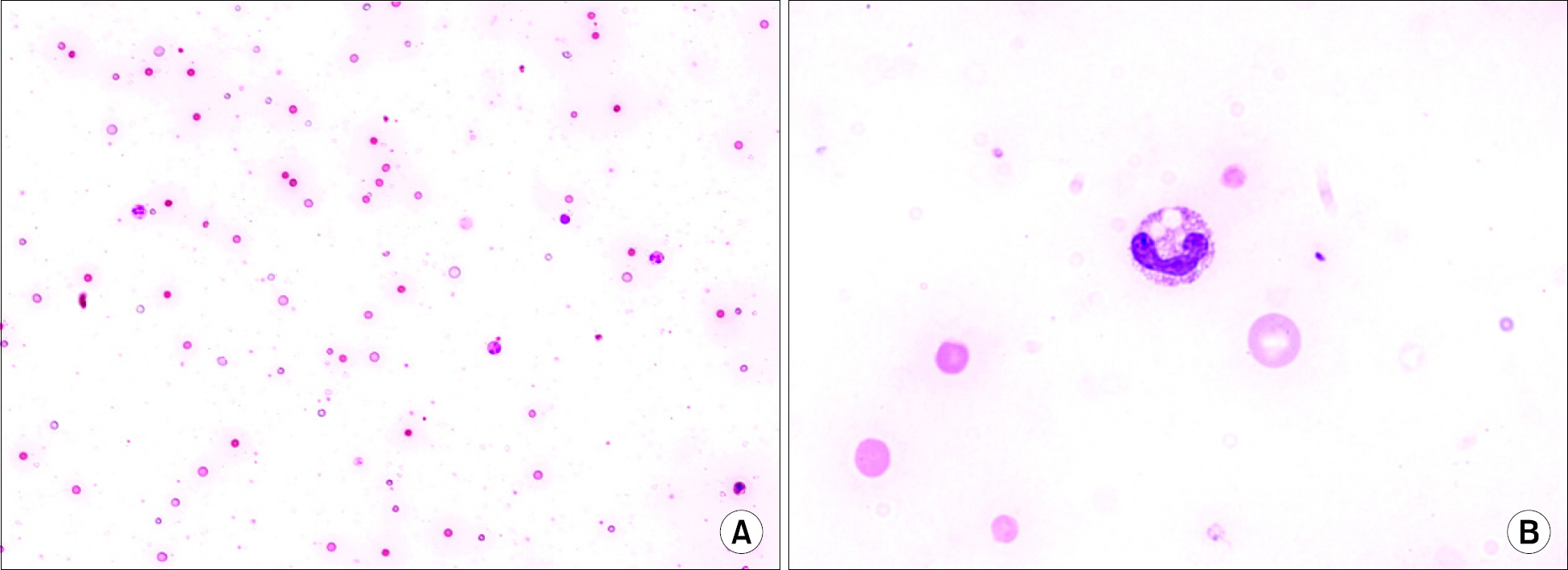
Fig. 2 The peripheral blood smear showed gross intravascular hemolysis with reddish background, a lot of irregular sized erythrocytes, many spherocytes, ghost erythrocytes, and toxic change in neutrophils with toxic vacuoles [(A) Wright-Giemsa stain, ×200; (B) Wright-Giemsa stain, ×1,000].
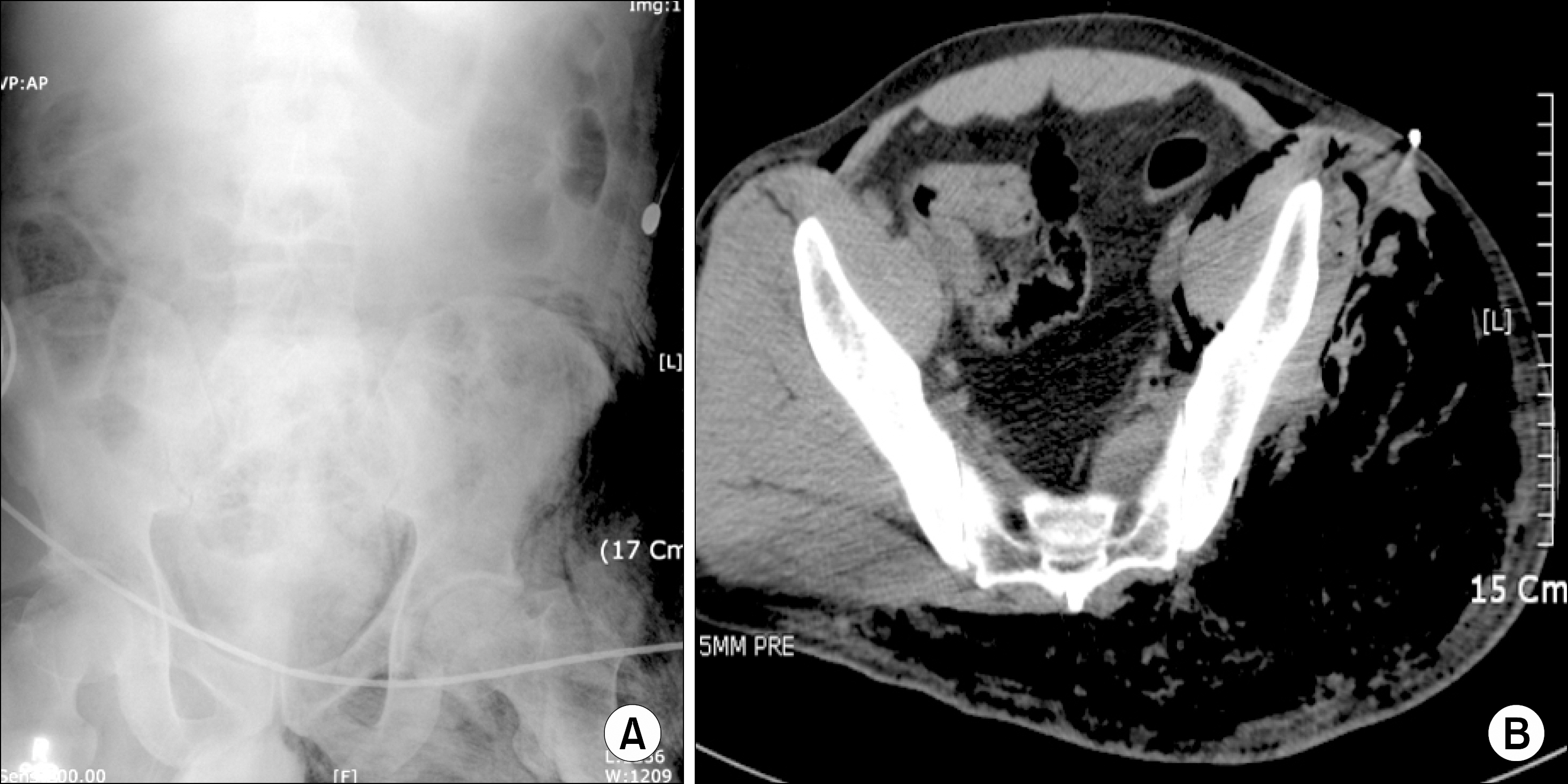
Fig. 3 Simple abdomen supine x-ray showed extensive subcutaneous emphysema on left side buttock and left inguinal area (A). Abdomen CT showed possible extensive gas gangrene and muscle destruction in the left buttock and left inguinal area (B).

Fig. 4 Gram stain showed gram positive bacilli (×1,000).
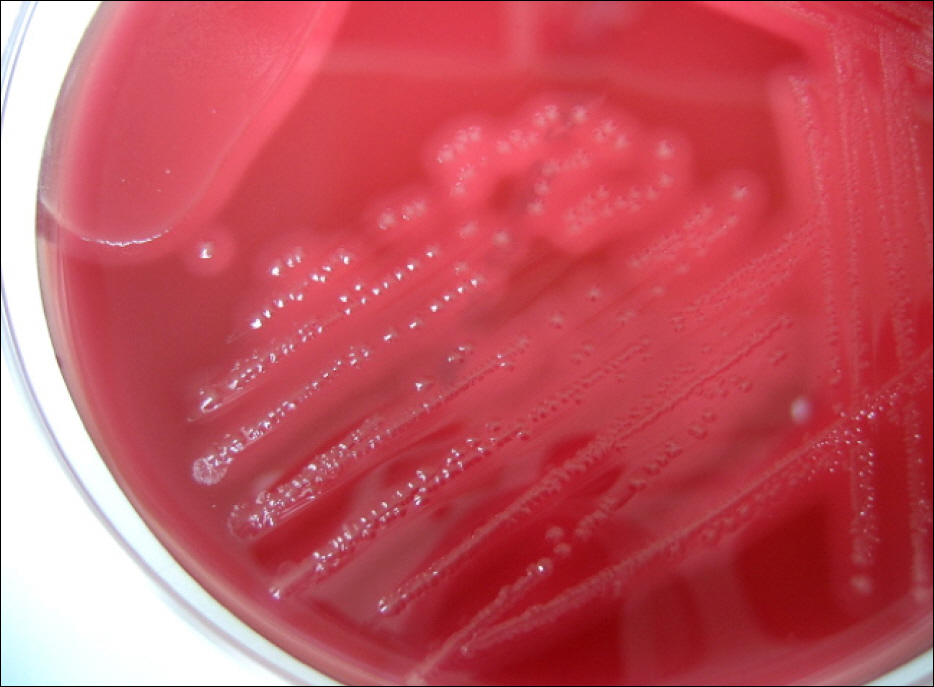
Fig. 5 Blood agar plate showed double zone of beta he-
Reference
-
1). Rechner PM., Agger WA., Mruz K., Cogbill TH. Clinical features of clostridial bacteremia: a review from a rural area. Clin Infect Dis. 2001. 33:349–53.
Article2). Haddy RI., Nadkarni DD., Mann BL, et al. Clostridial bacteremia in the community hospital. Scand J Infect Dis. 2000. 32:27–30.3). Vaiopoulos G., Calpadaki C., Sinifakoulis H, et al. Massive intravascular hemolysis: a fatal complication of Clostridium perfringens septicemia in a patient with acute myeloid leukemia. Leuk Lymphoma. 2004. 45:2157–9.
Article4). McArthur HL., Dalal BI., Kollmannsberger C. Intravascular hemolysis as a complication of Clostridium perfringens sepsis. J Clin Oncol. 2006. 24:2387–8.
Article5). Loran MJ., McErlean M., Wilner G. Massive hemolysis associated with Clostridium perfringens sepsis. Am J Emerg Med. 2006. 24:881–3.
Article6). Batge B., Filejski W., Kurowski V., Kluter H., Djonlagic H. Clostridial sepsis with massive intravascular hemolysis: rapid diagnosis and successful treatment. Intensive Care Med. 1992. 18:488–90.
Article7). Kuroda S., Okada Y., Mita M, et al. Fulminant massive gas gangrene caused by Clostridium perfringens. Intern Med. 2005. 44:499–502.
Article8). Abella BS., Kuchinic P., Hiraoka T., Howes DS. Atraumatic clostridial myonecrosis: case report and literature review. J Emerg Med. 2003. 24:401–5.
Article9). Poulou A., Manolis EN., Markou F., Ropotos A., Georgiadis M., Tsakris A. Fatal massive hemolysis as the first manifestation of Clostiridium perfringens septicemia in patient with non-systemic or local predisposing disorder. Anaerobe. 2007. 13:40–2.10). Singer AJ., Migdal PM., Oken JP., Chale SN., Moll UM. Clostridium perfringens septicemia with massive hemolysis in a patient with Hodgkin's lymphoma. Am J Emerg Med. 1997. 15:152–4.
Article11). Titball RW., Naylor CE., Basak AK. The Clostridium perfringens alpha-toxin. Anaerobe. 1999. 5:51–64.12). Stevens DL., Bryant AE. The role of clostridial toxins in the pathogenesis of gas gangrene. Clin Infect Dis. 2002. 35(1 Suppl):93–100.
Article13). Chen YM., Lee HC., Chang CM., Chuang YC., Ko WC. Clostridium bacteremia: emphasis on the poor prognosis in cirrhotic patients. J Microbiol Immunol Infect. 2001. 34:113–8.14). Ohtani S., Watanabe N., Kawata M., Harada K., Himei M., Murakami K. Massive intravascular hemolysis in a patient infected by a Clostridium perfringens. Acta Med Okayama. 2006. 60:357–60.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Clostridium perfringens Septicemia with Fatal Hemolytic Complication
- A Fulminant Case of Clostridium perfringens Septic Shock caused by a Liver Abscess with Massive Hemolytic Anemia
- Morganella Morganii Sepsis with Massive Hemolysis
- Massive intravascular hemolysis associated with Clostridium perfringens bacteremia
- Death due to Sepsis in Emphysematous Cholecystitis
