J Korean Acad Conserv Dent.
2011 Mar;36(2):149-153. 10.5395/JKACD.2011.36.2.149.
Partial pulp necrosis caused by excessive orthodontic force
- Affiliations
-
- 1Department of Conservative Dentistry, Yonsei University College of Dentistry, Microscope Center, Seoul, Korea. andyendo@yuhs.ac
- KMID: 2251820
- DOI: http://doi.org/10.5395/JKACD.2011.36.2.149
Abstract
- As the dental pulp is encased with a rigid, noncompliant shell, changes in pulpal blood flow or vascular tissue pressure can have serious implication for the health of pulp. Numerous studies have demonstrated that orthodontic force application may influence both blood flow and cellular metabolism, leading degenerative and/or inflammatory responses in the dental pulp. The aim of this case report is to present a case about tooth with chronic periapical abscess which showed normal vital responses. Excessive orthodontic force is thought to be the prime cause of partial pulp necrosis. Owing to remaining vital tissue, wrong dianosis can be made, and tooth falsely diagnosed as vital may be left untreated, causing the necrotic tissue to destroy the supporting tissuses. Clinician should be able to utilize various diagnostic tools for the precise diagnosis, and be aware of the endodontic-orthodontic inter-relationship.
Figure
-

Figure 1 Pre-operative clinical photo.

Figure 2 Pre-operative periapical x-ray.
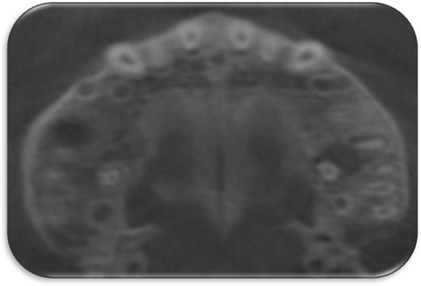
Figure 3 Pre-operative conebeam CT image. CT, computed tomograph.

Figure 4 Pre-operative conebeam CT image. CT, computed tomograph.
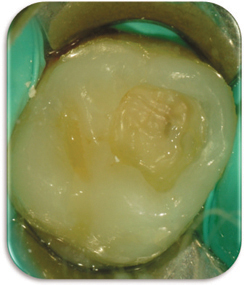
Figure 5 Cavity after IRM removal. IRM, intermediate restorative material.
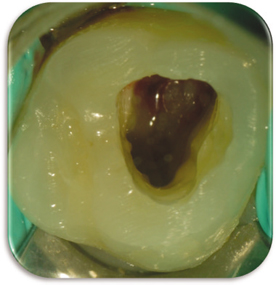
Figure 6 Pulp chamber immediate after access opening.

Figure 7 Periapical x-ray after canal filling.

Figure 8 6 month follow up-periapical x-ray.
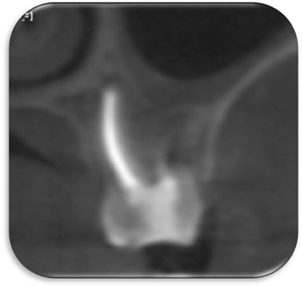
Figure 9 6 month follow up-conebeam CT image. CT, computed tomograph.
Reference
-
1. Nair PN. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med. 2004. 15:348–381.
Article2. Peters DD, Baumgartner JC, Lorton L. Adult pulpal diagnosis. I. Evaluation of the positive and negative responses to cold and electrical pulp tests. J Endod. 1994. 20:506–511.
Article3. Rowe AH, Pitt Ford TR. The assessment of pulpal vitality. Int Endod J. 1990. 23:77–83.
Article4. Küçükkeleş N, Okar I. Root resorption and pulpal changes due to intrusive force. J Marmara Univ Dent Fac. 1994. 2:404–408.5. Sano Y, Ikawa M, Sugawara J, Horiuchi H, Mitani H. The effect of continuous intrusive force on human pulpal blood flow. Eur J Orthod. 2002. 24:159–166.
Article6. Konno Y, Daimaruya T, Iikubo M, Kanzaki R, Takahashi I, Sugawara J, Sasano T. Morphologic and hemodynamic analysis of dental pulp in dogs after molar intrusion with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2007. 132:199–207.
Article7. Ramazanzadeh BA, Sahhafian AA, Mohtasham N, Hassanzadeh N, Jahanbin A, Shakeri MT. Histological changes in human dental pulp following application of intrusive and extrusive orthodontic forces. J Oral Sci. 2009. 51:109–115.
Article8. Tschamer H. Histology of dental pulp after activator treatment of late cases in adolescents. Zahnarztl Prax. 1974. 25:530–531.9. Hamilton RS, Gutmann JL. Endodontic-orthodontic relationships: a review of integrated treatment planning challenges. Int Endod J. 1999. 32:343–360.
Article10. Hamersky PA, Weimer AD, Taintor JF. The effect of orthodontic force application on the pulpal tissue respiration rate in the human premolar. Am J Orthod. 1980. 77:368–378.
Article11. Grossman LI. Origin of microorganisms in traumatized, pulpless, sound teeth. J Dent Res. 1967. 46:551–553.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A histologic study of pulpal reaction after experimental tooth movement in rats
- Dynamics of gingival crevicular fluid volume and enzyme activities after application of orthodontic force
- Corticotomy for orthodontic tooth movement
- Vital tooth with periapical lesion: spontaneous healing after conservative treatment
- Frictional forces in the fixed orthodontic appliance during tooth movement
