Clin Orthop Surg.
2015 Sep;7(3):351-358. 10.4055/cios.2015.7.3.351.
Evaluation of the Effusion within Biceps Long Head Tendon Sheath Using Ultrasonography
- Affiliations
-
- 1Department of Orthopedic Surgery, Armed Forces Capital Hospital, Seongnam, Korea.
- 2Department of Orthopedic Surgery, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. kysoos@catholic.ac.kr
- 3Department of Orthopedic Surgery, Nanoori Hospital, Incheon, Korea.
- KMID: 2234090
- DOI: http://doi.org/10.4055/cios.2015.7.3.351
Abstract
- BACKGROUND
Many shoulder diseases are related to glenohumeral joint synovitis and effusion. The purpose of the present study is to detect effusion within the biceps long head tendon sheath as the sign of glenohumeral joint synovitis using ultrasonography, and to evaluate the clinical meaning of effusion within the biceps long head tendon sheath.
METHODS
A consecutive series of 569 patients who underwent ultrasonography for shoulder pain were reviewed retrospectively and ultimately, 303 patients were included. The authors evaluated the incidence and amount of the effusion within the biceps long head tendon sheath on the ultrasonographic short axis view. Furthermore, the authors evaluated the correlation between the amount of effusion within the biceps long head tendon sheath and the range of motion and the functional score.
RESULTS
The effusion within the biceps long head tendon sheath was detected in 58.42% of the patients studied: 69.23% in adhesive capsulitis, 56.69% in rotator cuff tear, 41.03% in calcific tendinitis, and 33.33% in biceps tendinitis. The average amount of the effusion within the biceps long head tendon sheath was 1.7 +/- 1.6 mm, and it was measured to be the largest in adhesive capsulitis. The amount of effusion within biceps long head tendon sheath showed a moderate to high degree of correlation with the range of motion, and a low degree of correlation with the functional score and visual analogue scale for pain in each type of shoulder disease.
CONCLUSIONS
The effusion within the biceps long head tendon sheath is closely related to the range of motion and clinical scores in patients with painful shoulders. Ultrasonographic detection of the effusion within the biceps long head tendon sheath might be a simple and easy method to evaluate shoulder function.
Keyword
MeSH Terms
Figure
-
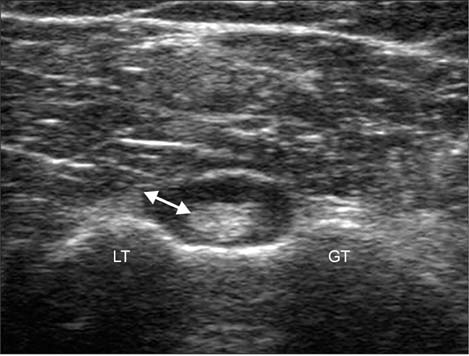
Fig. 1 Effusion within the biceps long head tendon sheath. The longest distance from the sheath to the tendon margin of the long head biceps tendon (arrow) was measured as the amount of the effusion within the biceps long head tendon sheath. GT: greater tubercle, LT: lesser tubercle.
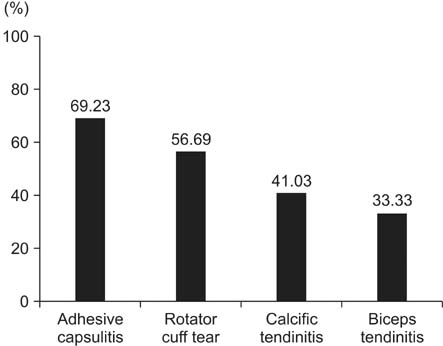
Fig. 2 The incidence of effusion within the biceps long head tendon sheath in each type of shoulder disease.

Fig. 3 The amount of effusion within the biceps long head tendon sheath in each type of shoulder disease.
Reference
-
1. Middleton WD. Ultrasonography of the shoulder. Radiol Clin North Am. 1992; 30(5):927–940.2. Hurt G, Baker CL Jr. Calcific tendinitis of the shoulder. Orthop Clin North Am. 2003; 34(4):567–575.
Article3. Shindle MK, Chen CC, Robertson C, et al. Full-thickness supraspinatus tears are associated with more synovial inflammation and tissue degeneration than partial-thickness tears. J Shoulder Elbow Surg. 2011; 20(6):917–927.
Article4. Saboeiro GR. Sonography in the treatment of calcific tendinitis of the rotator cuff. J Ultrasound Med. 2012; 31(10):1513–1518.
Article5. Yablon CM, Bedi A, Morag Y, Jacobson JA. Ultrasonography of the shoulder with arthroscopic correlation. Clin Sports Med. 2013; 32(3):391–408.
Article6. Al-Shawi A, Badge R, Bunker T. The detection of full thickness rotator cuff tears using ultrasound. J Bone Joint Surg Br. 2008; 90(7):889–892.
Article7. Iannotti JP, Ciccone J, Buss DD, et al. Accuracy of office-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears. J Bone Joint Surg Am. 2005; 87(6):1305–1311.
Article8. Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, Yamaguchi K. Detection and quantification of rotator cuff tears: comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am. 2004; 86(4):708–716.9. Koski JM. Axillar ultrasound of the glenohumeral joint. J Rheumatol. 1989; 16(5):664–667.10. Luukkainen R, Sanila MT, Luukkainen P. Poor relationship between joint swelling detected on physical examination and effusion diagnosed by ultrasonography in glenohumeral joints in patients with rheumatoid arthritis. Clin Rheumatol. 2007; 26(6):865–867.
Article11. Sanja MR, Mirjana ZS. Ultrasonographic study of the painful shoulder in patients with rheumatoid arthritis and patients with degenerative shoulder disease. Acta Reumatol Port. 2010; 35(1):50–58.12. Zubler V, Mamisch-Saupe N, Pfirrmann CW, Jost B, Zanetti M. Detection and quantification of glenohumeral joint effusion: reliability of ultrasound. Eur Radiol. 2011; 21(9):1858–1864.
Article13. Zuckerman JD, Rokito A. Frozen shoulder: a consensus definition. J Shoulder Elbow Surg. 2011; 20(2):322–325.
Article14. Oh JH, Kim SH, Lee HK, Jo KH, Bin SW, Gong HS. Moderate preoperative shoulder stiffness does not alter the clinical outcome of rotator cuff repair with arthroscopic release and manipulation. Arthroscopy. 2008; 24(9):983–991.
Article15. Hsu JE, Anakwenze OA, Warrender WJ, Abboud JA. Current review of adhesive capsulitis. J Shoulder Elbow Surg. 2011; 20(3):502–514.
Article16. Rodeo SA, Hannafin JA, Tom J, Warren RF, Wickiewicz TL. Immunolocalization of cytokines and their receptors in adhesive capsulitis of the shoulder. J Orthop Res. 1997; 15(3):427–436.
Article17. Ryu JD, Kirpalani PA, Kim JM, Nam KH, Han CW, Han SH. Expression of vascular endothelial growth factor and angiogenesis in the diabetic frozen shoulder. J Shoulder Elbow Surg. 2006; 15(6):679–685.
Article18. Neviaser JS. Adhesive capsulitis of the shoulder (the frozen shoulder). Med Times. 1962; 90(8):783–807.19. Gotoh M, Hamada K, Yamakawa H, et al. Perforation of rotator cuff increases interleukin 1beta production in the synovium of glenohumeral joint in rotator cuff diseases. J Rheumatol. 2000; 27(12):2886–2892.20. Lo IK, Marchuk LL, Hollinshead R, Hart DA, Frank CB. Matrix metalloproteinase and tissue inhibitor of matrix metalloproteinase mRNA levels are specifically altered in torn rotator cuff tendons. Am J Sports Med. 2004; 32(5):1223–1229.
Article21. Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg. 1997; 5(4):183–191.
Article22. Ahrens PM, Boileau P. The long head of biceps and associated tendinopathy. J Bone Joint Surg Br. 2007; 89(8):1001–1009.
Article23. Longo UG, Loppini M, Marineo G, Khan WS, Maffulli N, Denaro V. Tendinopathy of the tendon of the long head of the biceps. Sports Med Arthrosc. 2011; 19(4):321–332.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intratendinous Ganglion of the Long Head of the Biceps Tendon
- Subluxation of the Long Head Biceps Tendon Diagnosed by Dynamic Ultrasound
- Bilateral Congenital Absence of the Long Head of Biceps Brachii Tendon in Shoulder Joints: A case report
- Arthroscopic Treatment of the Intratendinous Ganglion of the Long Head of Biceps Brachii: A Case Report
- Accessory Tendon of Biceps Brachii Originated from Pectoralis Major
