Huge Left Ventricular Thrombus and Apical Ballooning associated with Recurrent Massive Strokes in a Septic Shock Patient
- Affiliations
-
- 1Department of Internal Medicine, Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea. khl2876@gmail.com
- 2Department of Neurology, Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Hongik Hospital, Seoul, Korea.
- KMID: 2227611
- DOI: http://doi.org/10.4266/kjccm.2016.31.1.39
Abstract
- The most feared complication of left ventricular thrombus (LVT) is the occurrence of systemic thromboembolic events, especially in the brain. Herein, we report a patient with severe sepsis who suffered recurrent devastating embolic stroke. Transthoracic echocardiography revealed apical ballooning of the left ventricle with a huge LVT, which had not been observed in chest computed tomography before the stroke. This case emphasizes the importance of serial cardiac evaluation in patients with stroke and severe medical illness.
Keyword
Figure
-
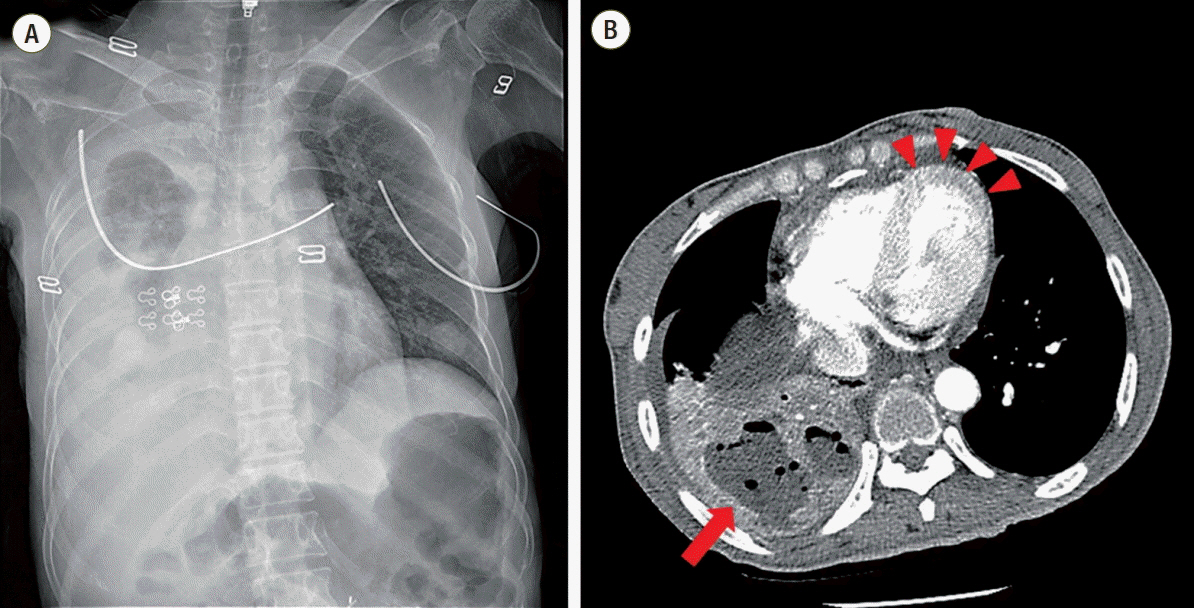
Fig. 1. Chest radiographic examination at initial admission. Chest X-ray (A) showed right lung consolidation, which was identified as lung abscess in chest computed tomography (red arrow) (B). There was no abnormality of cardiac contour and no visible mural thrombus in the left ventricle (red arrowheads).
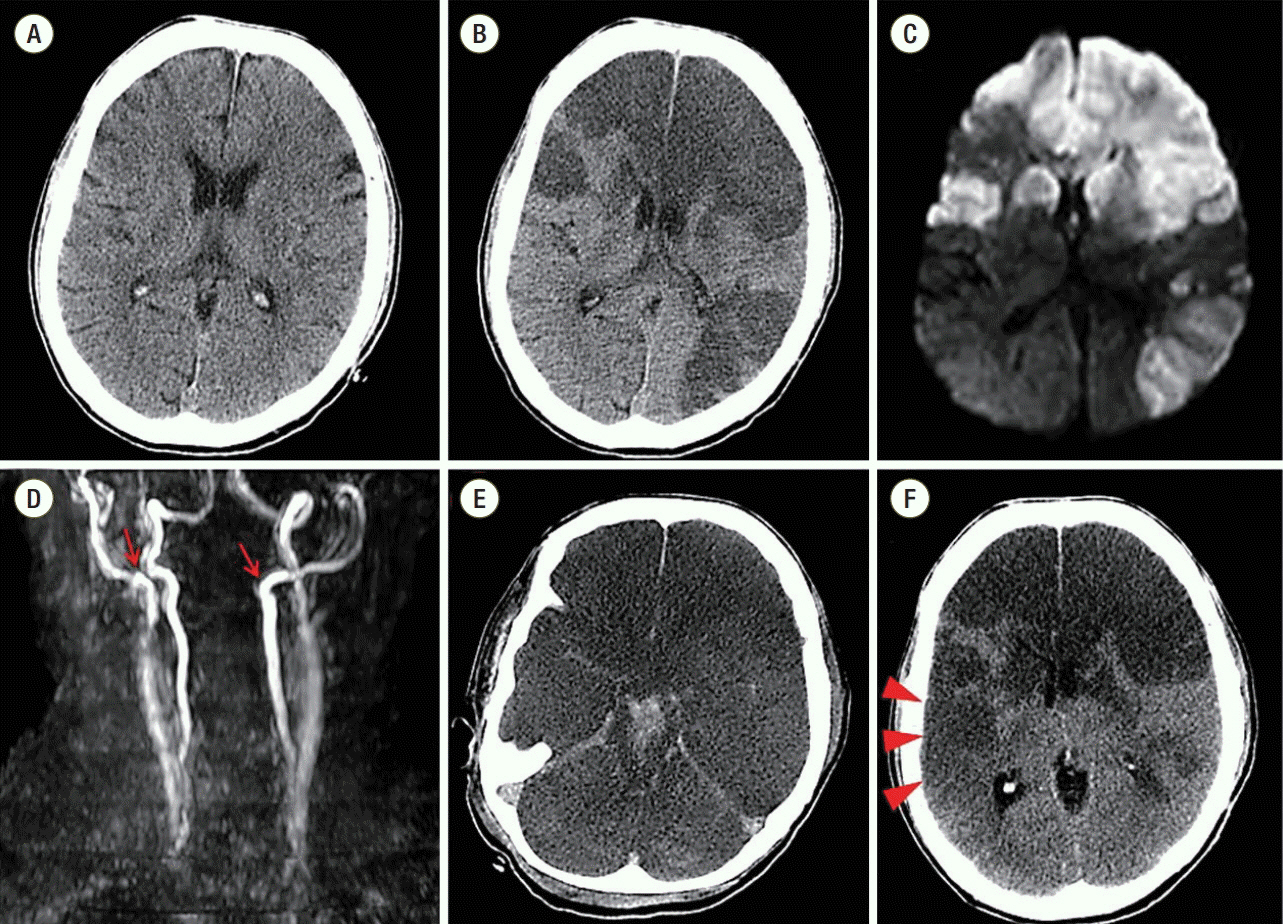
Fig. 2. The results of brain imaging studies. Normal brain computed tomographic findings at initial admission (A). Large multiple territorial infarctions were shown in brain computed tomography (hypo-attenuated lesions) (B) and diffusion-weighted magnetic resonance imaging (high signal intensities) (C) during stupor. There was total occlusion of the proximal portions of both internal carotid arteries (red arrows) (D). Combined brain stem and intraventricular hemorrhages (hyper-attenuated lesions) were shown (E). In serial examinations, a new acute infarction was seen in the right temporal lobe (red arrowheads) in brain computed tomography (F).
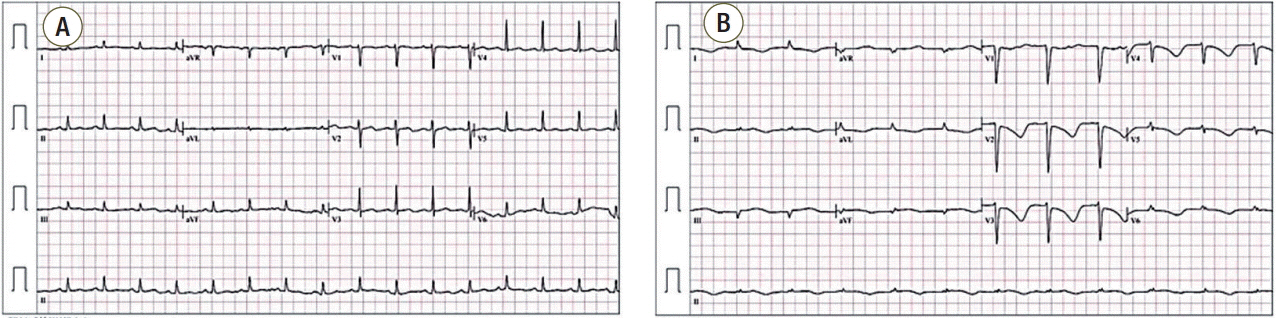
Fig. 3. Electrocardiographic changes. During the stroke, electrocardiogram showed newly developed T inversions in multiple leads (B) compared to the exam at initial admission (A).

Fig. 4. Echocardiographic findings. Transthoracic echocardiography showed a large mural thrombus at the apex of the left ventricle (red arrowheads). Wall contraction at the base and mid-portion of the left ventricle was relatively preserved during systole compared to that of the left ventricular apex.
Cited by 1 articles
-
Major Trauma induced Left Ventricular Thrombus after Acute Myocardial Infarction
Dong Wook Lee, Ju Hee Ha, Jun Ho Kim, Ki Beom Park, Jae Joon Lee, Han Il Choi, Jin Hee Kim
J Lipid Atheroscler. 2016;5(2):163-167. doi: 10.12997/jla.2016.5.2.163.
Reference
-
References
1. de Gregorio C. Cardioembolic outcomes in stress-related cardiomyopathy complicated by ventricular thrombus: a systematic review of 26 clinical studies. Int J Cardiol. 2010; 141:11–7.
Article2. Leick J, Szardien S, Liebetrau C, Willmer M, Fischer-Rasokat U, Kempfert J, et al. Mobile left ventricular thrombus in left ventricular dysfunction: case report and review of literature. Clin Res Cardiol. 2013; 102:479–84.
Article3. Komamura K, Fukui M, Iwasaku T, Hirotani S, Masuyama T. Takotsubo cardiomyopathy: pathophysiology, diagnosis and treatment. World J Cardiol. 2014; 6:602–9.
Article4. Madias JE. Why the current diagnostic criteria of Takotsubo syndrome are outmoded: a proposal for new criteria. Int J Cardiol. 2014; 174:468–70.
Article5. Pelliccia F, Greco C, Vitale C, Rosano G, Gaudio C, Kaski JC. Takotsubo syndrome (stress cardiomyopathy): an intriguing clinical condition in search of its identity. Am J Med. 2014; 127:699–704.
Article6. Antonucci E, Fiaccadori E, Donadello K, Taccone FS, Franchi F, Scolletta S. Myocardial depression in sepsis: from pathogenesis to clinical manifestations and treatment. J Crit Care. 2014; 29:500–11.
Article7. Singh K, Carson K, Shah R, Sawhney G, Singh B, Parsaik A, et al. Meta-analysis of clinical correlates of acute mortality in takotsubo cardiomyopathy. Am J Cardiol. 2014; 113:1420–8.
Article8. Y-Hassan S, Settergren M, Henareh L. Sepsis-induced myocardial depression and takotsubo syndrome. Acute Card Care. 2014; 16:102–9.
Article9. Srichai MB, Junor C, Rodriguez LL, Stillman AE, Grimm RA, Lieber ML, et al. Clinical, imaging, and pathological characteristics of left ventricular thrombus: a comparison of contrast-enhanced magnetic resonance imaging, transthoracic echocardiography, and transesophageal echocardiography with surgical or pathological validation. Am Heart J. 2006; 152:75–84.
Article10. Leurent G, Larralde A, Boulmier D, Fougerou C, Langella B, Ollivier R, et al. Cardiac MRI studies of transient left ventricular apical ballooning syndrome (takotsubo cardiomyopathy): a systematic review. Int J Cardiol. 2009; 135:146–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Persistent Apical Ballooning Complicated by Apical Thrombus in Takotsubo Cardiomyopathy of Systemic Lupus Erythematosus Patient
- Takotsubo Cardiomyopathy: A Case of Persistent Apical Ballooning Complicated by an Apical Mural Thrombus
- A Case of Consecutive Right and Left Ventricular Dysfunction
- A case of transient mid-ventricular ballooning syndrome
- Magnetic Resonance Imaging of Transient Left Ventricular Apical Ballooning Related to Emotional Stress: a Case Report
