Korean J Crit Care Med.
2016 Feb;31(1):25-33. 10.4266/kjccm.2016.31.1.25.
Trends in the Use of Intensive Care by Very Elderly Patients and Their Clinical Course in a Single Tertiary Hospital in Korea
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea. sangmin2@snu.ac.kr
- 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
- KMID: 2227609
- DOI: http://doi.org/10.4266/kjccm.2016.31.1.25
Abstract
- BACKGROUND
The number of elderly patients admitted to intensive care units (ICUs) is growing with the increasing proportion of elderly persons in the Korean general population. It is often difficult to make decisions about ICU care for elderly patients, especially when they are in their 90s. Data regarding the proportion of elderly patients in their 90s along with their clinical characteristics in ICU are scarce.
METHODS
The records of Korean patients > or = 90 years old who were admitted to the medical ICU in a tertiary referral hospital between January 2005 and December 2014 were retrospectively reviewed. We compared the trend in ICU use and characteristics of these elderly patients between 2005-2009 and 2010-2014.
RESULTS
Among 6,186 referred patients, 55 aged > or = 90 years were admitted to the medical ICU from 2005 to 2014. About 58.2% of these patients were male, and their mean age was 92.7 years. Their median Charlson comorbidity index score was 2 (IQR 1-3) and their mean APACHE II score was 25.0 (IQR 19.0-34.0). The most common reason for ICU care was acute respiratory failure. There were no differences in the survival rates between the earlier and more recent cohorts. However, after excluding patients who had specified "do not resuscitate" (DNR), the more recent group showed a significantly higher survival rate (53.8% mortality for the earlier group and 0% mortality for the recent group). Among the survivors, over half were discharged to their homes. More patients in the recent cohort (n=26 [78.8%]) specified DNR than in the earlier cohort (n=7 [35.0%], p=0.004). The number and proportion of patients > or = 90 years old among patients using ICU during the 2005-2014 study period did not differ.
CONCLUSIONS
The use of ICU care by elderly patients > or = 90 years old was consistent from 2005-2014. The overall mortality rate tended to decrease, but this was not statistically significant. However, the proportion of patients specifying DNR was higher among more recent patients, and the recent group showed an even better survivorship after sensitivity analysis excluded patients specifying DNR.
Keyword
MeSH Terms
Figure
-

Fig. 1. The proportion of patients who were aged ≥ 90 years among whole patients during study period and that of the patients who agreed to DNR among them. DNR: do not resuscitate.
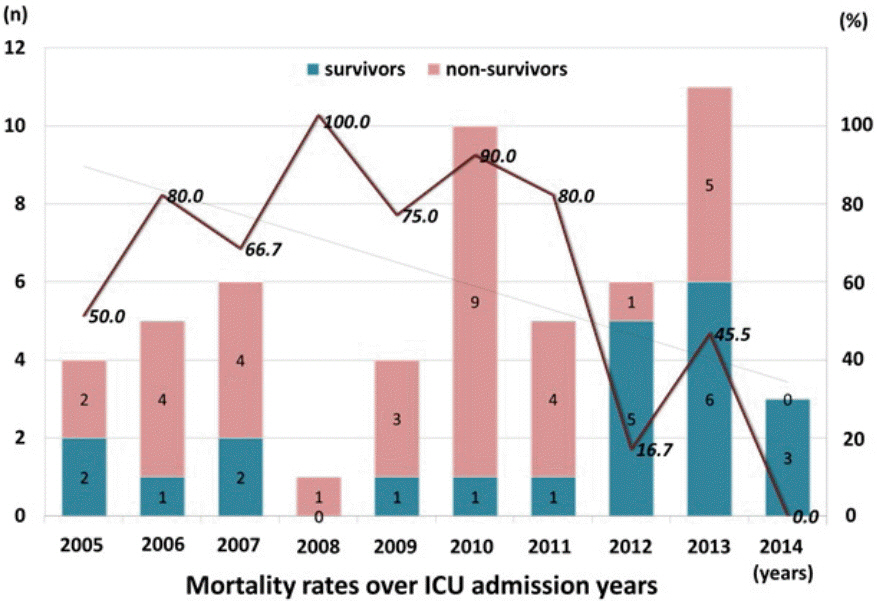
Fig. 2. Mortality rates over years of ICU admission among study population (patients aged ≥ 90 years). ICU: intensive care unit.
Cited by 1 articles
-
Characteristics and prognostic factors of very elderly patients admitted to the intensive care unit
Song-I Lee, Younsuck Koh, Jin Won Huh, Sang-Bum Hong, Chae-Man Lim
Acute Crit Care. 2022;37(3):372-381. doi: 10.4266/acc.2022.00066.
Reference
-
References
1. Blot S, Cankurtaran M, Petrovic M, Vandijck D, Lizy C, Decruyenaere J, et al. Epidemiology and outcome of nosocomial bloodstream infection in elderly critically ill patients: a comparison between middle-aged, old, and very old patients. Crit Care Med. 2009; 37:1634–41.
Article2. Nguyen YL, Angus DC, Boumendil A, Guidet B. The challenge of admitting the very elderly to intensive care. Ann Intensive Care. 2011; 1:29.
Article3. Vosylius S, Sipylaite J, Ivaskevicius J. Determinants of outcome in elderly patients admitted to the intensive care unit. Age Ageing. 2005; 34:157–62.
Article4. Statistics Korea. Statistics of elderly in Korea 2014. 2014.5. Sim YS, Jung H, Shin TR, Kim DG, Park SM. Mortality and outcomes in very elderly patients 90 years of age or older admitted to the ICU. Respiratory Care. 2015; 60:347–55.
Article6. Engelhardt HT Jr, Rie MA. Intensive care units, scarce resources, and conflicting principles of justice. JAMA. 1986; 255:1159–64.
Article7. Holt AW, Vedig AE. Do advance care directives improve acute care services for older people? Med J Aust. 2006; 185:406.
Article8. Yayan J. Trends in intensive care in patients over 90 years of age. Clin Interv Aging. 2012; 7:339–47.
Article9. Duke GJ, Barker A, Knott CI, Santamaria JD. Outcomes of older people receiving intensive care in Victoria. Med J Aust. 2014; 200:323–6.
Article10. Yu W, Ash AS, Levinsky NG, Moskowitz MA. Intensive care unit use and mortality in the elderly. J Gen Intern Med. 2000; 15:97–102.
Article11. Roch A, Wiramus S, Pauly V, Forel JM, Guervilly C, Gainnier M, et al. Long-term outcome in medical patients aged 80 or over following admission to an intensive care unit. Crit Care. 2011; 15:R36.
Article12. Rellos K, Falagas ME, Vardakas KZ, Sermaides G, Michalopoulos A. Outcome of critically ill oldest-old patients (aged 90 and older) admitted to the intensive care unit. J Am Geriatr Soc. 2006; 54:110–4.
Article13. Casey CM, Scholar P, Happ MB. Assessment and management of older adults with complex illness in the critical care unit. American Association of Critical Care Nurses. 2007.14. Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991; 100:1619–36.15. Bagshaw SM, Webb SA, Delaney A, George C, Pilcher D, Hart GK, et al. Very old patients admitted to intensive care in Australia and New Zealand: a multi-centre cohort analysis. Crit Care. 2009; 13:R45.
Article16. Lee K, Jang HJ, Hong SB, Lim CM, Koh Y. Do-not-resuscitate order in patients, who were deceased in a medical intensive care unit of an university hospital in Korea. Korean J of Crit Care Med. 2008; 23:84–96.
Article17. Sinuff T, Cook DJ, Rocker GM, Griffith LE, Walter SD, Fisher MM, et al. DNR directives are established early in mechanically ventilated intensive care unit patients. Can J Anaesth. 2004; 51:1034–41.
Article18. Bacchetta MD, Eachempati SR, Fins JJ, Hydo L, Barie PS. Factors influencing DNR decision-making in a surgical ICU. J Am Coll Surg. 2006; 202:995–1000.
Article19. Huang YC, Huang SJ, Ko WJ. Survey of do-not-resuscitate orders in surgical intensive care units. J Formos Med Assoc. 2010; 109:201–8.
Article20. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985; 13:818–29.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcomes of very elderly (≥ 80 years) critical-ill patients in a medical intensive care unit of a tertiary hospital in Korea
- Interhospital Comparison of Outcome from Intensive Care Unit with APACHE III Scoring System
- Factors Influencing Intensive Care Unit Nurses’ Competency in Delirium Care in A Tertiary General Hospital
- Demographic Changes in Intensive Care Units in Korea over the Last Decade and Outcomes of Elderly Patients: A Single-Center Retrospective Study
- Comparison of End-of-Life Care Intensity between Cancer and Non-cancer Patients: a Single Center Experience
