Korean Circ J.
2008 Jan;38(1):43-50. 10.4070/kcj.2008.38.1.43.
Rates and Related Factors of Progression to Hypertension among Prehypertensive Local Residents Aged 45 or Over in Chuncheon City: Hallym Aging Study from a Community-Based Cross-Sectional Study
- Affiliations
-
- 1Internal Medicine, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Korea.
- 2Division of Cardiology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Korea. kshong@hallym.ac.kr
- 3Department of Family Medicine, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Korea.
- 4Division of Endocrinology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Korea.
- 5Hallym Institute for Aging Research, Hallym University, Korea.
- 6Speech, Language and Hearing Sciences, University of Arizona, Arizona, USA.
- 7Department of Social and Preventive Medicine, Hallym University College of Medicine, Chuncheon, Korea.
- KMID: 2225873
- DOI: http://doi.org/10.4070/kcj.2008.38.1.43
Abstract
- BACKGROUND AND OBJECTIVES
Prehypertension (preHT) is considered to a precursor of hypertension and it is a predictor of excessive cardiovascular risk. We investigated the rates and determinants of progression to hypertension (HT) among local residents aged 45 or over, and we compared the differences in demographic factors, anthropometric measurements, life styles and metabolic profiles between the progression individuals and non-progression individuals.
SUBJECTS AND METHODS
Data from the Hallym Aging Study, which was conducted 3 years apart were used to form the sample of 489 adults. PreHT was defined by the Joint National Committee (JNC-7) criteria. We conducted interviews to determine the life style (alcohol, smoking and exercise) and the measured obesity indices. The metabolic profiles were fasting blood sugar (FBS), cholesterol, triglyceride and high density lipoprotein (HDL)-Cholesterol. The factors related to progression to HT were examined by using multiple logistic regression analysis.
RESULTS
The progression rate to HT was 56.4% (56.9% in men, 55.9% in women). The presence of metabolic syndrome was significantly greater and the body mass index (BMI) and systolic blood pressure were significantly higher in the progression group compared with the non-progression group (p=0.0475, p=0.0099, p=0.0082, respectively). Important determinants of progression to HT are a BMI> or =25 kg/m(2) [odds ratio (OR): 2.26, 95% confidence interval (CI): 1.02-5.22] and a diastolic blood pressure of 85-89 mmHg (OR: 6.11, CI: 1.55-24.13). Changes of FBS (deltaFBS) and pulse pressure (deltaPP) according to a time interval of 3 years are the significant related factors (OR: 3.40, CI: 1.04-11.13 and OR: 9.40, CI: 2.19-40.12, respectively).
CONCLUSION
PreHT frequently progresses to HT over a period of 3 years. A higher BMI and diastolic blood pressure at the index survey are significantly related to progression. deltaFBS and deltaPP are also important determinants. Therefore, early recognition of preHT and intensive life style modification are needed to prevent progression to HT.
Keyword
MeSH Terms
Figure
-
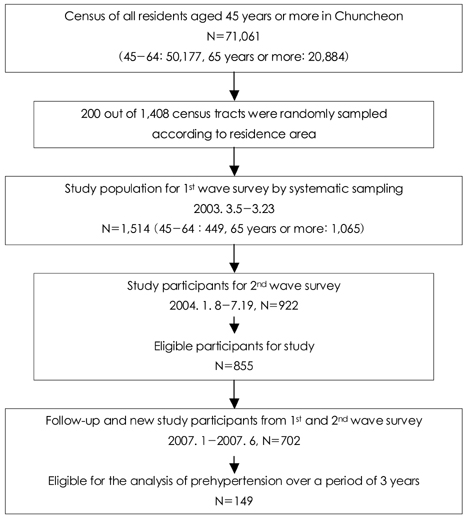
Fig. 1 Flow chart of the study population for Hallym Aging Study.
Reference
-
1. Izzo JL, Black HR, editors. Hypertension Premier. 2003. 3rd ed. Baltimore: Lippincott Williams and Wilkins;235–238.2. Suh I. Risk of death in men with normal of high-normal blood pressure. Circulation. 2002. 106:Suppl. 760.3. Seo IL, Kim HC, Ahn SB, et al. Korea Institute for Health and Social Affaires. National Health and nutrition examination in Korea, 2005. Ministry of Health and Welfare. 2007. 37–41.4. Kim HJ, Ahn YA, Chun HI, Lee JS, Huh SC, Kim ST. Epidemiological studies on geriatric hypertension in Korea. Korean Circ J. 1984. 14:327–332.5. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevevtion, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003. 42:1206–1252.6. Levy RL, Hillman CC, Stroud WD, White PD. Transient hypertension: its significance in terms of later development of sustained hypertension and cardiovascular-renal diseases. JAMA. 1944. 126:829–833.7. Julius S, Schork MA. Borderline hypertension: a critical review. J Chronic Dis. 1971. 23:723–754.8. Leitschuh M, Cupples LA, Kannel W, Gagnon D, Chobanianl A. High-normal blood pressure progression to hypertension in the Framingham Heart Study. Hypertension. 1991. 17:22–27.9. Vasan RS, Larson MG, Leip EP, Kannel WB, Levy D. Assessment of frequency of progression to hypertension in non-hypertensive participants in the Framingham Heart Study: a cohort study. Lancet. 2001. 358:1682–1686.10. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002. 360:1903–1913.11. Vasan RS, Larson MG, Leip EP, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001. 345:1291–1297.12. Qureshi AI, Suri MF, Kirmani JF, Divani AA, Mohammad Y. Is prehypertension a risk factor for cardiovascular disease? Stroke. 2005. 36:1859–1863.13. Qureshi AI, Suri MF, Kirmani JF, Divani AA, Mohammad Y. Prevalence and trends of prehypertension and hypertension in United States: National Health and Nutrition Examination Surveys 1976 to 2000. Med Sci Monit. 2005. 11:CR403–CR409.14. Kshirsagar AV, Carpenter M, Bang H, Wyatt SB, Colindres RE. Blood pressure usually considered normal is associated with an elevated risk of cardiovascular disease. Am J Med. 2006. 119:133–141.15. Greenlund KJ, Croft JB, Mensah GA. Prevalence of heart disease and stroke risk factors in persons with prehypertension in the United States, 1999-2000. Arch Intern Med. 2004. 164:2113–2118.16. Zhang Y, Lee EF, Devereux RB, et al. Prehypertension, diabetes, and cardiovascular disease risk in a population-based sample. Hypertension. 2006. 47:410–414.17. Liszka HA, Mainous AG 3rd, King DE, Everett CJ, Egan BM. Prehypertension and cardiovascular morbidity. Ann Fam Med. 2005. 3:294–299.18. Wang Y, Wang OJ. The prevalence of prehypertension and hypertension among US adults according to the new joint national committee guidelines. Arch Intern Med. 2004. 164:2126–2134.19. Lee JE, Kim YG, Choi YH, Huh W, Kim DJ, Oh HY. Serum uric acid is associated with microalbuminuria in prehypertension. Hypertension. 2006. 47:962–967.20. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Rreport of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001. 285:2486–2497.21. Jee SH, Suh I, Kim IS, Appel LJ. Smoking and atherosclerotic cardiovascular disease in men with low levels of serum cholesterol. JAMA. 1999. 282:2149–2155.22. Joint National Committee. Sixth report of the Joint National Committee on Prevevtion, Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med. 1997. 157:2413–2446.23. Washio M, Tokunaga S, Yoshimasu K, et al. Role of prehypertension in the development of coronary atherosclerosis in Japan. J Epidemiol. 2004. 14:57–62.24. Rodriguez BL, Labarthe DR, Huang B, Lopez-Gomez J. Rise of blood pressure with age: new evidence of population differences. Hypertension. 1994. 24:779–785.25. Julius S, Nesbitt SD, Egan BM, et al. Feasibility of treating prehypertension with an angiotensin-receptor blocker. N Engl J Med. 2006. 354:1685–1697.26. Hong KS, Jeong JY, Jang SN, et al. The prevalence and related risk factors of prehypertension among local residents aged 45 or over in Chuncheon city. Korean Circ J. 2006. 36:535–542.27. Stamler J. Epidemiologic findings on body mass and blood pressure in adults. Ann Epidemiol. 1991. 1:347–362.28. Cordero A, Laclaustra M, Leon M, et al. Prehypertension is associated with insulin resistance state and not with an initial renal function impairment. Am J Hypertens. 2006. 19:189–196.29. Mainous AG 3rd, Everett CJ, Liszka H, King DE, Egan BM. Prehypertension and mortality in a nationally representative cohort. Am J Cardiol. 2004. 94:1496–1500.30. Tsai PS, Ke TL, Huang CJ, et al. Prevalence and determinants of prehypertension status in the Taiwanese general population. J Hypertens. 2005. 23:1355–1360.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Prevalence and Related Risk Factors of Prehypertension among Local Residents Aged 45 or Over in Chuncheon City: The Hallym Aging Study (A Community-Based Cross-Sectional Study)
- Factors Affecting the Depressive Mood Experience in Local Residents: Focusing on Gangseo-gu, Seoul
- The Prevalence and Risk Factors of the Metabolic Syndrome among Local Residents Aged 45 or over in Chuncheon: Hallym Aging Study
- Impact of the Utilization Gap of the Community-Based Smoking Cessation Programs on the Attempts for Quitting Smoking between Wonju and Chuncheon Citizen
- Prevalence of Knee Pain and Its Influence on Quality of Life and Physical Function in the Korean Elderly Population: A Community Based Cross-Sectional Study
