Probable Left Atrial Myxoma Presenting as Concurrent Cerebral and Myocardial Infarctions
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Soonchunhyang University, Cheonan Hospital, Cheonan, Korea. lovelee93@hanmail.net
- 2Department of Internal Medicine, St. Mary's Hospital, Cheongju, Korea.
- KMID: 2225712
- DOI: http://doi.org/10.4070/kcj.2008.38.11.622
Abstract
- Concurrent cerebral and coronary artery embolization is a theoretically possible, but extremely rare complication of an atrial myxoma. We present a paitent with a left atrial mass (a probable myxoma) who presented with concurrent cerebral and myocardial infarctions due to emboli of tumor origin. An 84-year-old woman presented with an acute cerebral infarction of the middle cerebral artery territory. Several hours after admission, she complained of chest pain consistent with a myocardial infarction. Transthoracic and transesophageal echocardiographic studies revealed the presence of a large, mobile, heteroechoic mass with a few daughter nodules in the left atrium, compatible with a myxoma. Coronary angiography disclosed subtotal occlusion of the ramus intermedius branch and visible tumor vascularization adjacent to the right coronary artery. With medical treatment, including anticoagulation, the patient was stabilized and had an uneventful clinical course for the ensuing 6 months since discharge.
Keyword
MeSH Terms
Figure
-
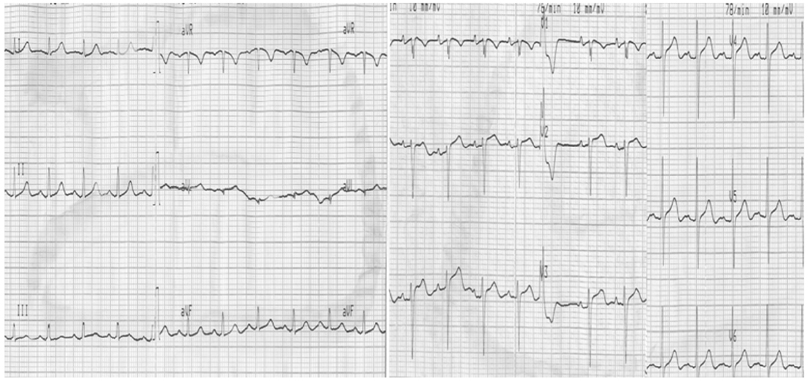
Fig. 1 Initial ECG showed intermittent ventricular premature complexes and diffuse non-specific ST segment changes. ECG: electrocardiogram.
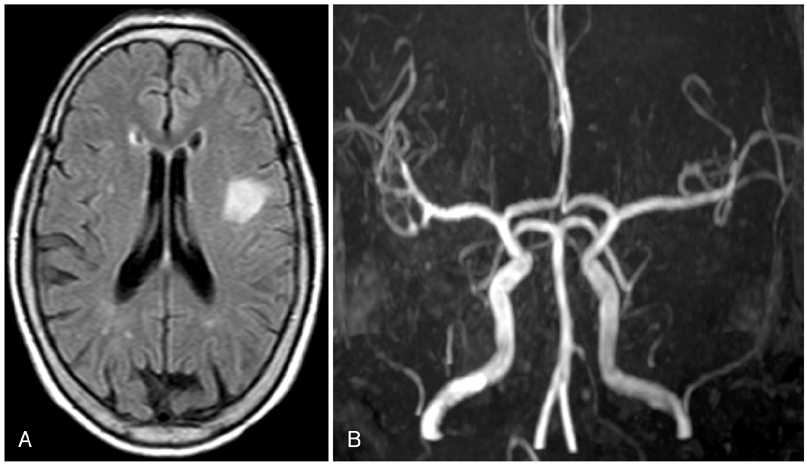
Fig. 2 Initial brain MR images. A: T2 flair MRI image showing left MCA territory infarction. B: brain MR angiogram showing no significant stenosis of the cerebral artery. MCA: middle cerebral artery.

Fig. 3 Transthoracic and transesophageal echocardiographic studies. A: transthoracic echocardiogram (apical four-chamber view) revealing the presence of a large mass with heterogenic echogenicity in the left atrium, possibly indicative of atrial myxoma. B: transesophageal echocardiogram of the mass shows irregular surface, with a polypoid nodule.
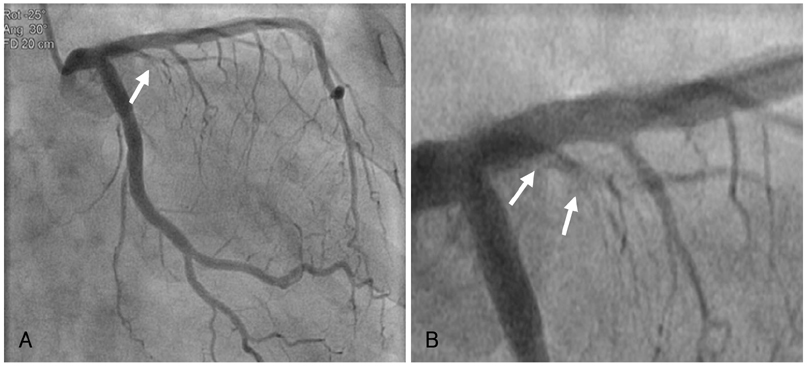
Fig. 4 Coronary angiography in right anterior oblique view (A) and enlarged image (B) showing subtotal occlusion of ramus intermedius with thrombi-like hazziness (arrows).
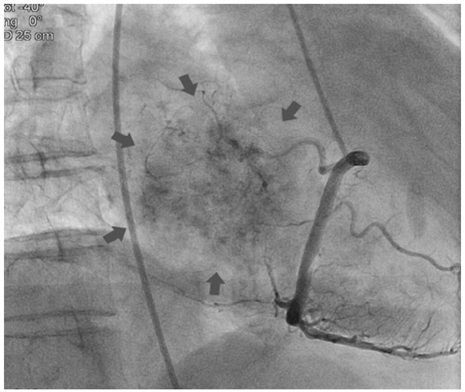
Fig. 5 Visible feeding vascularization originating from the right coronary artery (arrows), strongly suggestive of cardiac myxoma.
Reference
-
1. Goswami KC, Shrivastava S, Bahl VK, Saxena A, Manchanda SC, Wasir HS. Cardiac myxomas: clinical and echocardiographic profile. Int J Cardiol. 1998. 63:251–259.2. Reynen K. Cardiac myxomas. N Engl J Med. 1995. 333:1610–1617.3. Rhim HY, Youn HJ, Park JW, et al. Clinical experience of cardiac myxoma. Korean Circ J. 1999. 29:1317–1323.4. Bjessmo S, Ivert T. Cardiac myxoma: 40 years' experience in 63 patients. Ann Thorac Surg. 1997. 63:697–700.5. Lee VH, Connolly HM, Brown RD Jr. Central nervous system manifestations of cardiac myxoma. Arch Neurol. 2007. 64:1115–1120.6. Lee CK, Seo JK, Kim DY, et al. A case of left atrial myxoma presenting with myocardial infarction. Korean Circ J. 2004. 34:512–515.7. Panos A, Kalangos A, Sztajzel J. Left atrial myxoma presenting with myocardial infarction: case report and review of the literature. Int J Cardiol. 1997. 62:73–75.8. Kanemitsu S, Takao M, Fujinaga K, et al. A case of surgically treated left atrial myxoma following acute multiple embolism including cerebral embolism. Kyobu Geka. 2001. 54:147–150.9. Frenay JJ, Bonte J, Franken P, Henuzet C, Telerman M, Primo G. Left atrial myxoma with left retinal emboli, right hemiparesis and myocardial infarction: neurologic and echocardiographic diagnosis: surgical treatment. Acta Neurol Belg. 1981. 81:215–222.10. Romisher SC, Cannon LA, Davakis N. Atrial myxoma associated with inferior myocardial infarction. Ann Emerg Med. 1991. 20:1236–1238.11. Shapiro LM. Cardiac tumours: diagnosis and management. Heart. 2001. 85:218–222.12. Meng Q, Lai H, Lima J, Tong W, Qian Y, Lai S. Echocardiographic and pathologic characteristics of primary cardiac tumors: a study of 149 cases. Int J Cardiol. 2002. 84:69–75.13. Demir M, Akpinar O, Acarturk E. Atrial myxoma: an unusual cause of myocardial infarction. Tex Heart Inst J. 2005. 32:445–447.14. Ha JW, Kang WC, Chung N, et al. Echocardiographic and morphologic characteristics of left atrial myxoma and their relation to systemic embolism. Am J Cardiol. 1999. 83:1579–1582.15. Braun S, Schrftter H, Reynen K, Schwencke C, Strasser RH. Myocardial infarction as complication of left atrial myxoma. Int J Cardiol. 2005. 101:115–121.16. Marshall WH Jr, Steiner RM, Wexler L. 'Tumor vascularity' in left atrial myxoma demonstrated by selective coronary arteriography. Radiology. 1969. 93:815–816.17. Shimono T, Makino S, Kanamori Y, Kinoshita T, Yada I. Left atrial myxomas: using gross anatomic tumor types to determine clinical features and coronary angiographic findings. Chest. 1995. 107:674–679.18. Roudaut R, Labbe T, Lorient-Roudaut MF, et al. Mechanical cardiac valve thrombosis: is fibrinolysis justified? Circulation. 1992. 86:5 Suppl. 8–15.19. Abascal VM, Kasznica J, Aldea G, Davidoff R. Left atrial myxoma and acute myocardial infarction: a dangerous duo in the thrombolytic agent era. Chest. 1996. 109:1106–1108.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Left Atrial Myxomoa Presented as Pseudovasculitis
- The Report of One Case with the Left Atrial Myxoma Complicated with the Cerebral Embolism
- A Case of Left Atrial Myxoma Presenting with Myocardial Infarction
- Recurred Right Atrial Myxoma after Resection of Left Atrial Myxoma (Recurred Myxoma): A case report
- A Case of Left Atrial Myxoma Presenting as Acute Pulmonary Edema
