Korean Circ J.
2011 Mar;41(3):167-170. 10.4070/kcj.2011.41.3.167.
Recurrent Infective Endocarditis Associated With Pyogenic Spondylodiskitis
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Hanyang University, Guri Hospital, Guri, Korea. kimsg@hanyang.ac.kr
- KMID: 2225134
- DOI: http://doi.org/10.4070/kcj.2011.41.3.167
Abstract
- Infective endocarditis is a life-threatening condition caused by microbial infection of the heart's endocardial surface. This condition can also be associated with bacterial infections of other organs. We experienced an unusual case of recurrent infective endocarditis associated with pyogenic spondylodiskitis. A 70-year-old man presented with persistent fever and lower back pain visited our hospital. The patient had a past history of recurrent infective endocarditis. He was diagnosed with infective endocarditis again based on clinical symptoms and echocardiographic findings. Magnetic resonance imaging was used to evaluate lower back pain, which showed acute spondylodiskitis on L3 and L4 vertebrae. The patient completely recovered following four weeks of antibiotic therapy.
Keyword
MeSH Terms
Figure
-
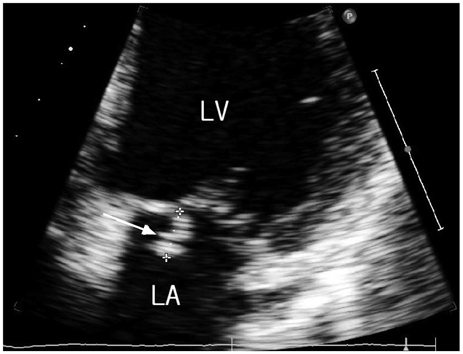
Fig. 1 A 2.7×1.4 cm sized vegetation on the posterior leaflet of mitral valve.
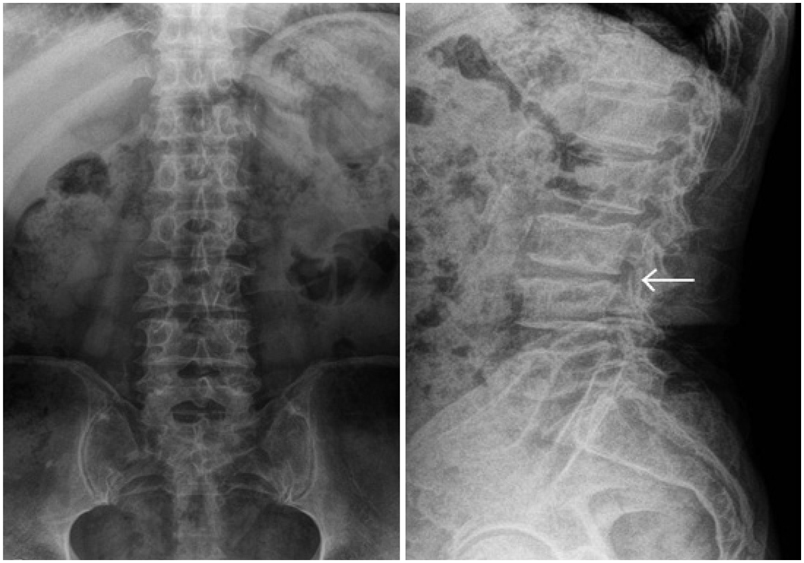
Fig. 2 Plain radiograph shows narrowing of the disc space at L3-L4 level. Destruction of the superior endplate of the L4 vertebra, and the inferior endplate of L3 vertebra is seen (arrow).

Fig. 3 Spine MRI shows abnormal high signal density in the disc within the adjacent vertebral bodies at L3-L4 level (arrow). Bony destruction of vertebral bodies is seen in L3 and L4.
Reference
-
1. Hopkinson N, Stevenson J, Benjamin S. A case ascertainment study of septic discitis: clinical, microbiological and radiological features. QJM. 2001. 94:465–470.2. Cottle L, Riordan T. Infectious spondylodiscitis. J Infect. 2008. 56:401–412.3. Ponte CD, McDonald M. Septic discitis resulting from Escherichia coli urosepsis. J Fam Pract. 1992. 34:767–771.4. Park CB, Kim JJ, Song JK, et al. Right-Sided Infective Endocarditis in Korea. Korean Circ J. 2005. 35:633–638.5. Moreillon P, Que YA. Infective endocarditis. Lancet. 2004. 363:139–149.6. Duval X, Leport C. Prophylaxis of infective endocarditis: current tendencies, continuing controversies. Lancet Infect Dis. 2008. 8:225–232.7. Kim MK, Song JK, Kang DH, et al. Recent trends and clinical outcomes of infective endocarditis. Korean J Med. 2000. 58:28–38.8. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007. 116:1736–1754.9. Yi MZ, Lee SH, Park CB, et al. Clinical characteristics of nosocomial infective endocarditis in a tertiary referral hospital. Korean Circ J. 2006. 36:236–241.10. Talsania N, Ogundipe O. Infective discitis mimicking infective endocarditis and osteoarthritic back pain. Internet J Rheumatol. 2005. 2:3.11. Udayaraj UP, Gendi NS, Osman EM. Septic discitis as a complication of infective endocarditis caused by Streptococcus oralis. J Rheumatol. 2003. 30:632–633.12. Pigrau C, Almirante B, Flores X, et al. Spontaneous pyogenic vertebral osteomyelitis and endocarditis: incidence, risk factors, and outcome. Am J Med. 2005. 118:1287.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pyogenic Arthritis of the Shoulder in Patient with Infective Endocarditis: A Case Report
- A Case of Infective Endocarditis Occurred during Treatment for Infectious Spondylitis Accompanied by Peptostreptococcus Anaerobius Bacteremia
- A Case of Infective Endocarditis with Mycotic Aneurysms
- Streptococcus Spondylitis Concomitant Infectious Endocarditis: A Case Report
- A case of Libman-Sacks endocarditis confused with infective endocarditis
