Hybrid Approach for the Treatment of Thoracic Aortic Arch Aneurysm in a Patient With Chronic Obstructive Lung Disease and Retrosternal Adhesion
- Affiliations
-
- 1Division of Cardiology, Eulji University Hospital, Daejeon, Korea. sahnglee@eulji.ac.kr
- 2Division of Thoracic and Cardiovascular Surgery, Eulji University Hospital, Daejeon, Korea.
- KMID: 2225108
- DOI: http://doi.org/10.4070/kcj.2011.41.7.413
Abstract
- A 73-year-old woman with a history of chronic hypertension and severe chronic obstructive pulmonary disease, presented to a district general hospital with thoracic pain in a profound state of shock. She was diagnosed with cardiac tamponade, severe mitral regurgitation, and Stanford type A (Debakey type I) intramural hematoma. Her ascending aorta was of a significant size and therefore emergent repair was done to replace the ascending aorta and mitral valve. After 6 months, an increased aneurysmal size of 6.0 cm was observed in a follow up contrast-enhanced computed tomography angiography. The patient was successfully treated by a staged hybrid procedure involving initial supra-aortic reconstruction.
MeSH Terms
Figure
-
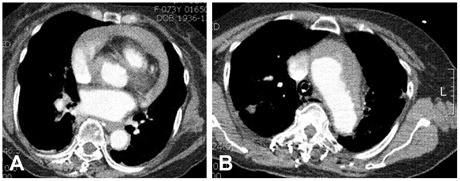
Fig. 1 The aorta CTA at initial presentation. The CT scan showed a large pericardial effusion (A) and Stanford type A (Debakey type I) intramural hematoma (B). CTA: computed tomography angiography.
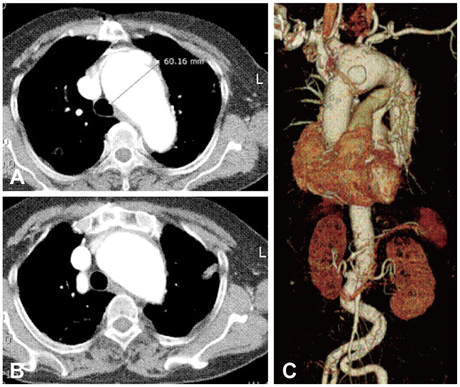
Fig. 2 The aorta CTA after 6 months. The CT scan showed an increase in aneurysmal size from 4.3 cm to 6.0 cm (A). It also showed retrosternal adhesions of arch aneurysm and manubrium of the sternum (B). The innominate artery itself was aneurysmal (C). CTA: computed tomography angiography.
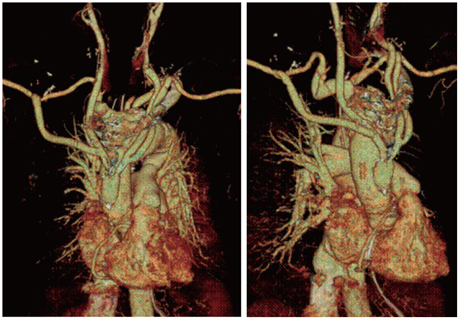
Fig. 3 The aorta CTA one week after the de-brancing procedure. The CT scan showed that the circulation was maintained in right-left CCAs and right-left SCA. CTA: computed tomography angiography, CCA: common carotid artery, SCA: subclavian artery.
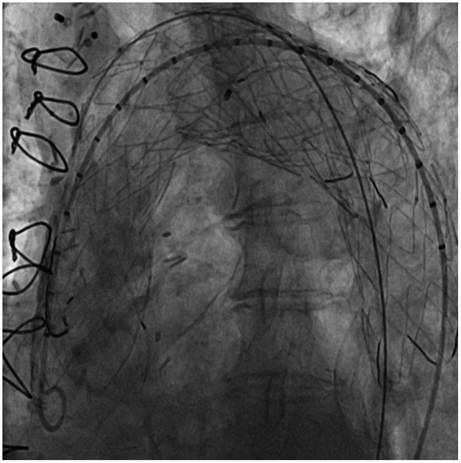
Fig. 4 Angiography during the stenting of the descending thoracic aorta. A 38×150 mm and 40-38-100 mm tapered SEAL thoracic stent graft (S&G Biotech INC., Seongnam, Korea) were deployed to cover the full length of the aneurysm.
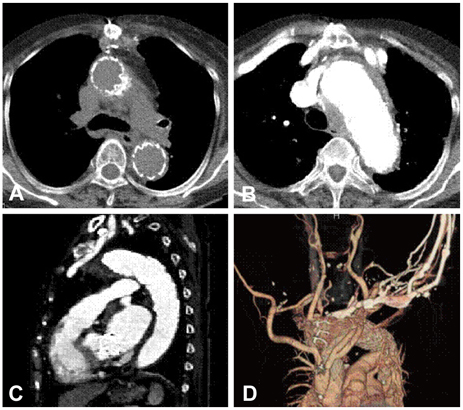
Fig. 5 The aorta CTA one week after stenting of the descending thoracic aorta. The CT scan showed stent graft covering ascending aorta (A)-aortic arch (B)-proximal descending thoracic aorta. It also showed mural thrombus outside of the stent-graft. There was no evidence of contrast leakage from the anastomosis site of the graft and aortic arch (C). Bypass grafts from the ascending aorta to the bilateral CCA and SCA were patent (D). CTA: computed tomography angiography, CCA: common carotid artery, SCA: subclavian artery.
Reference
-
1. Alsac JM, Coscas R, Paraskevas N, Francis F, Castier Y, leseche G. Acute debranching and stent grafting for a ruptured penetrating ulcer of the aortic arch. Ann Vasc Surg. 2009. 23:687.e5–687.e8.2. Pressler V, McNamara JJ. Thoracic aortic aneurysm: natural history and treatment. J Thorac Cardiovasc Surg. 1980. 79:489–498.3. Perko MJ, Norgaard M, Herzog M, Olsen PS, Schröder TV, Pettersson G. Unoperated aortic aneurysms: a survey of 170 patients. Ann Thorac Surg. 1995. 59:1204–1209.4. Pressler V, McNamara JJ. Aneurysms of the thoracic aorta. J Thorac Cardiovasc Surg. 1985. 89:50–54.5. de Bakey ME, McCollum CH, Graham JM. Surgical treatment of aneurysms of the descending thoracic aorta: long-term results in 500 patients. J Cardiovasc Surg (Torino). 1978. 19:571–576.6. Livesay JJ, Cooley DA, Ventemiglia RA, et al. Surgical experience in descending thoracic aneurysmectomy with and without adjuncts to avoid ischeamia. Ann Thorac Surg. 1985. 39:37–46.7. Borst HG, Jurmann M, Bühner B, Laas J. Risk of replacement of descending aorta with a standardized left bypass technique. J Thorac Cardiovasc Surg. 1994. 107:126–133.8. von Segesser LK, Killer I, Jenny R, Lutz U, Turina MI. Improved distal circulatory support for repair of descending thoracic aortic aneurysms. Ann Thorac Surg. 1993. 56:1373–1380.9. Shim WH. Hybrid approach for complex thoracic aortic pathology. Korean Circ J. 2010. 40:368–369.10. Sayed S, Thompson MM. Endovascular repair of the descending thoracic aorta: evidence for change in clinical practice. Vascular. 2005. 13:148–157.11. Kang WC, Shin EK, Ahn TH, et al. Combined open endovascular repair for aortic arch pathology. Korean Circ J. 2010. 40:399–404.12. Koullias GJ, Wheatley GH 3rd. State-of-the-art of hybrid procedures for the aortic arch: a meta-analysis. Ann Thorac Surg. 2010. 90:689–697.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hybrid Method for Stent-graft Insertion in a Patient with a Thoracic Aortic Aneurysm Involving the Aortic Arch: A case report
- Hybrid Procedure for Aortic Arch Repair: Arch Vessels Debranching with Supraaortic Revascularization Followed by Endovascular Aortic Stent Grafting
- One-Stage Ascending, Arch, and Descending Thoracic Aorta Replacement Through Median Sternotomy
- Hybrid Procedure for Aortic Arch Aneurysm: Arch Vessels Debranching and Thoracic Endovascular Aortic Repair?: 2 case reports
- Visceral Debranching Thoracic Endovascular Aneurysm Repair for Chronic Dissecting Thoracoabdominal Aortic Aneurysm
