Intermediate and Long-Term Results of Transcatheter Closure of Patent Foramen Ovale Using the Amplatzer Patent Foramen Ovale Occluder: One Case of Pulmonary Embolism Irrespective of Patent Foramen Ovale Closure
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, Hallym University, Anyang, Korea. cdj915@hanmail.net
- KMID: 2225098
- DOI: http://doi.org/10.4070/kcj.2011.41.7.356
Abstract
- BACKGROUND AND OBJECTIVES
Patent foramen ovale (PFO) has been implicated in the pathogenesis of cryptogenic stroke or transient ischemic attack (TIA) due to paradoxical embolism, and in the pathogenesis of migraine. This paper reports the intermediate and long-term results of transcatheter closure of PFO associated with cerebrovascular accidents (CVAs), TIAs and migraine, using the Amplatzer PFO occluder. This paper also reports a case of pulmonary embolism which developed in one patient after PFO closure.
SUBJECTS AND METHODS
From January 2003 to May 2010, 16 patients with PFO (seven males and nine females) with a history of at least one episode of cryptogenic stroke/TIA, CVA, or migraine and who underwent percutaneous transcatheter closure of PFO using the Amplatzer occluder. All the procedures were performed under general anesthesia and were assisted by transesophageal echocardiography.
RESULTS
The device was implanted without any significant complications in all the patients, and the PFOs were effectively closed. At an average follow-up period of 54 months, the 15 patients with TIA/CVA had no recurrence of any thromboembolic event. The symptoms in one patient with migraine subsided after occlusion of the PFO. In this study, pulmonary embolism occurred five months after PFO closure in one patient, but the cause of pulmonary embolism was not identified. However, it is believed that the pulmonary embolism occurred without stroke recurrence because occlusion of the PFO was performed when the patient had a stroke event.
CONCLUSION
It can be concluded that according to the intermediate and long-term follow-up results, transcatheter PFO closure is an effective and safe therapeutic modality in the prevention of thromboembolic events, especially in the patients with cryptogenic stroke/TIA, and PFO closure is helpful in the treatment of migraine. However, this study involved a small number of patients and also the follow-up period was not long enough. Hence, randomized, controlled trials are necessary to determine if this approach is preferable to medical therapy for the prevention of recurrent stroke or as primary treatment for patients with migraine headache.
MeSH Terms
Figure
-
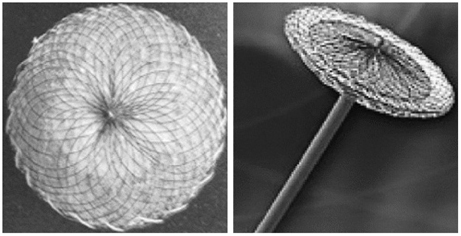
Fig. 1 Amplatzer PFO occluder (AGA Medical Corporation) is a self expandable, double disc device made from Nitinol wire mesh. The two discs are linked together by a short connecting waist allowing free motion of each disc.

Fig. 2 PFO occlusion using the Amplatzer PFO occluder. A: the selective superior vena cava angiography after the implantation of Amplatzer PFO occluder (arrow). B: the simple chest radiography, lateral view 5 months after PFO closure (arrow). PFO: patent foramen ovale.
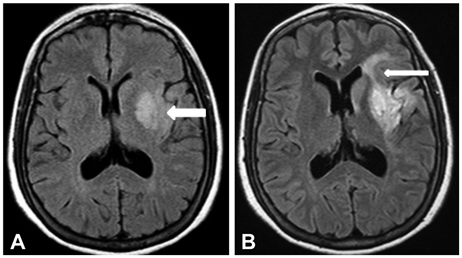
Fig. 3 Recurrence stroke was detected on an MRI scan. A: 1st acute infarction in the left middle cerebral artery-left frontotemporal lobe, insular cortex, and basal ganglia (arrow). B: 2nd acute infarction (2 months later)-left frontal lobe (arrow).
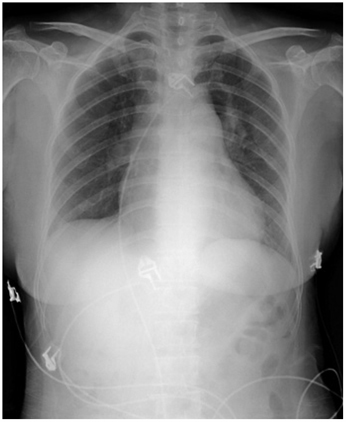
Fig. 4 Chest X-ray (sitting position) shows prominent right hilum and decreased pulmonary vascularity when the patient was admitted again via emergency room with dyspnea, five months after the patent foramen ovale closure.
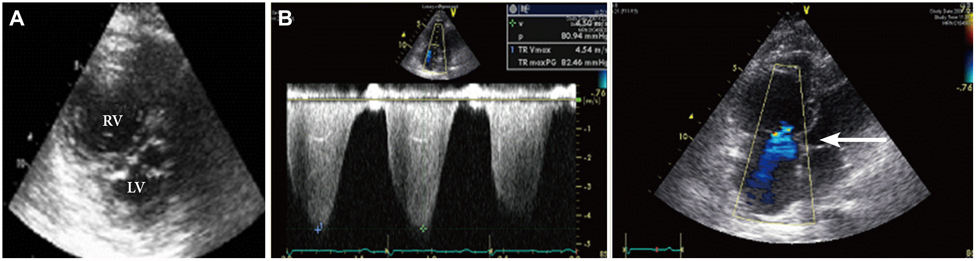
Fig. 5 Patients' 2D echocardiogram revealed severe pulmonary hypertension, right ventricular dysfunction, and tricuspid regurgitation. A: the 2D echocardiogram (2 chamber view) revealed right ventricular dysfunction (right ventricle is larger than the left ventricle). B: pulmonary hypertension and tricuspid regurgitation (arrow). 2D: 2-dimensional, RV: right ventricle, LV: left ventricle.
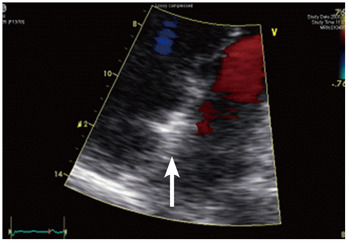
Fig. 6 When the patient was admitted again via emergency room with dyspnea, five months after PFO closure, neither thromboembolism nor shunt was observed in this case treated using the Amplatzer PFO occluder (arrow). PFO: patent foramen ovale.
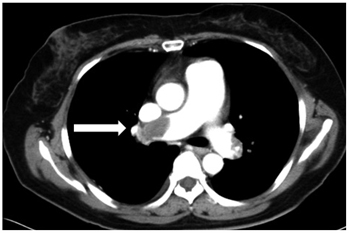
Fig. 7 Chest CT angiography shows acute pulmonary embolism (arrow).
Reference
-
1. Di Tullio M, Sacco RL, Gopal A, Mohr JP, Homma S. Patent foramen ovale as a risk factor for cryptogenic stroke. Ann Intern Med. 1992. 117:461–465.2. Diener HC, Weimar C, Katsarava Z. Patent foramen ovale: paradoxical connection to migrane and stroke. Curr Opin Neurol. 2005. 18:299–304.3. Oh BH, Park SW, Choi YJ, et al. Prevalence of the patent foramen ovale in young patients with ischemic cerebrovascular disease: transesophageal contrast echocardiographic study. Korean Circ J. 1993. 23:217–222.4. Meissner I, Whisnant JP, Khandheria BK, et al. Prevalence of potential risk factors for stroke assessed by transesophageal echocardiography and carotid ultrasonography: the SPARC study. Stroke Prevention: Assessment of Risk in a Community. Mayo Clin Proc. 1999. 74:862–869.5. Homma S, Sacco RL, Di Tullio MR, Sciacca RR, Mohr JP. Effect of medical treatment in stroke patients with patent foramen ovale: patent foramen ovale in Cryptogenic Stroke Study. Circulation. 2002. 105:2625–2631.6. Bogousslavsky J, Garazi S, Jeanrenaud X, Aebischer N, Van Melle G. Lausanne Stroke with Paradoxal Embolism Study Group. Stroke recurrence in patients with patent foramen ovale: the Lausanne Study. Neurology. 1996. 46:1301–1305.7. Mas JL, Zuber M. French Study Group on Patent Foramen Ovale and Atrial Septal Aneurysm. Recurrent cerebrovascular events in patients with patent foramen ovale, atrial septal aneurysm, or both and cryptogenic stroke or transient ischemic attack. Am Heart J. 1995. 130:1083–1088.8. Agmon Y, Khandheira BK, Meissner I, et al. Frequency of atrial septal aneurysms in patients with cerebral ischemic events. Circulation. 1999. 99:1942–1944.9. Chun KJ. Patent foramen ovale and cryptogenic stroke. Korean Circ J. 2008. 38:631–637.10. De Castro S, Cartoni D, Fiorelli M, et al. Morphological and functional characteristics of patent foramen ovale and their embolic implications. Stroke. 2000. 31:2407–2413.11. Kerut EK, Norfleet WT, Plotnick GD, Giles TD. Patent foramen ovale: a review of associated conditions and the impact of physiological size. J Am Coll Cardiol. 2001. 38:613–623.12. Gaspardone A, Iani C, Papa M. Percutaneous closure of patent foramen ovale: awise approach. G Ital Cardiol (Rome). 2008. 9:593–602.13. Mattioli A, Bonetti L, Aquilina M, Oldani A, Longhini C, Mattioli G. Association between atrial septal aneurysm and patent foramen ovale in young patients with recent stroke and normal carotid arteries. Cerebrovasc Dis. 2003. 15:4–10.14. Lamy C, Giannesini C, Zuber M, et al. Clinical and imaging findings in cryptogenic stroke patients with and without patent foramen ovale: the PFO-ASA Study. Atrial Septal Aneurysm. Stroke. 2002. 33:706–711.15. Overell JR, Bone I, Less KR. Interatrial septal abnormalities and stroke: a meta-analysis of case-control studies. Neurology. 2000. 55:1172–1179.16. Onorato E, Melzi G, Casilli F, et al. Patent foramen ovale with paradoxical embolism: mid-term results of transcatheter closure in 256 patients. J Interv Cardiol. 2003. 16:43–50.17. Windecker S, Wahl A, Chatterjee T, et al. Percutaneous closure of patent foramen ovale in patients with paradoxical embolism: long-term risk of recurrent thromboembolic events. Circulation. 2000. 101:893–898.18. Du ZD, Cao QL, Joseph A, et al. Transcatheter closure of patent foramen ovale in patients with paradoxical embolism: intermediate-term risk of recurrent neurological events. Catheter Cardiovasc Interv. 2002. 55:189–194.19. Bruch L, Parsi A, Grad MO, et al. Transcatheter closure of interatrial communications for secondary prevention of paradoxical embolism: single center experience. Circulation. 2002. 105:2845–2848.20. Meier B. Closure of patent foramen ovale: technique, pitfalls, complications, and follow up. Heart. 2005. 91:444–448.21. Morandi E, Anzola GP, Angeli S, Melzi G, Onorato E. Transcatheter closure of patent foramen ovale: a new migraine treatment. J Interv Cardiol. 2003. 16:39–42.22. Wilmshurst PT, Nightingale S, Walsh KP, Morrison WL. Effect on migraine of closure of cardiac right-to-left shunts to prevent recurrence of decompression illness or stroke or for haemodynamic reasons. Lancet. 2000. 356:1648–1651.23. Stewart WF, Shetcher A, Rasmussen BK. Migraine prevalence: a review of population-based studies. Neurology. 1994. 44:6 Suppl 4. S17–S23.24. Migraine-Nimodipine European Study Group M. European multicenter trial of nimodipine in the prophylaxis of common migraine (migraine without aura). Headache. 1989. 29:633–638.25. Migraine-Nimodipine European Study Group M. European multicenter trial of nimodipine in the prophylaxis of classic migraine (migraine with aura). Headache. 1989. 29:639–642.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT Diagnosis of Paradoxical Embolism via a Patent Foramen Ovale in a Patient with a Pulmonary Embolism and Prominent Eustachian Valve
- A New Method for Patent Foramen Ovale Closure: Delivering Sheath Over Coronary Sinus Catheter into Left Atrium
- Transcatheter Closure of Patent Foramen Ovale in a Stroke Patient under the Guidance of Transesophageal Echocardiography
- Thrombus in Transit within a Patent Foramen Ovale: Gone with the Cough!
- Transcatheter Treatment of Patent Foramen Ovale Combined with Abnormal Drainage of Left Superior Vena Cava to Left Upper Pulmonary Vein
