Transcatheter Closure of Atrial Septal Defect: Does Age Matter?
- Affiliations
-
- 1Division of Pediatric Cardiology, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea. cjy0122@yuhs.ac
- KMID: 2225069
- DOI: http://doi.org/10.4070/kcj.2011.41.11.633
Abstract
- Atrial septal defect (ASD) is the most common type of common congenital heart disease (CHD) in adults. During the last decade, there has been a remarkable change in the treatment strategy of ASD, shifting the therapeutic gold standard from surgery to transcatheter closure, along with refinements and the evolution of device technology. Reports on the outcome of transcatheter ASD closure have shown an excellent efficacy as well as a low complication rate. However, the procedural details and/or outcomes of this procedure may be influenced by several factors including morphologic characteristics of the defect, co-morbid diseases, as well as individual factors including age and weight of the patient. Because the risk-benefit relationship in both the very young and the elderly subsets of the patients has not been clearly defined yet, closure of an ASD with device may be potentially subtracted from the treatment option in these patient groups. In this article, we will review the basis for device closure in small children and elderly patients with ASD and provide an overview of the frequently encountered problems.
Keyword
Figure
-
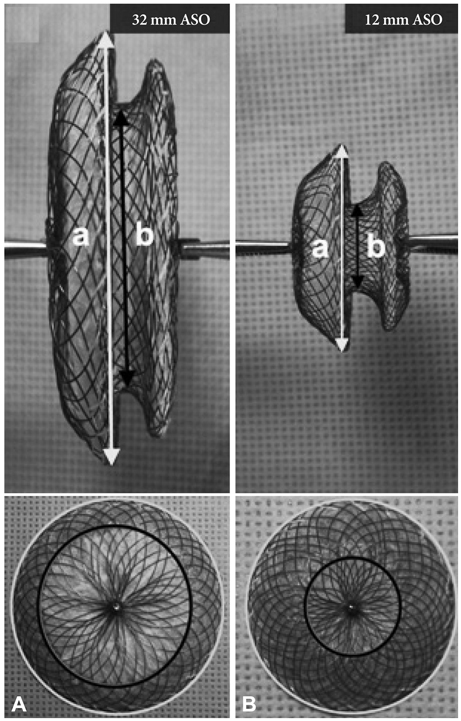
Fig. 1 Discrepancy in the left atrial disc and waist ratio (a/b). This figure shows that in 32 mm ASO, the (a) and (b) ratio is 1.44, but in a 12 mm ASO, the (a) and (b) ratio is 2.17. Relative large rim of LA disc in smaller devices may encroach to adjacent cardiac structures which prevent safe device closure. In reality, these are entirely different devices, when considering the structure and shape. Therefore, the discrepancy maximizes as the device gets smaller. LA disc is marked. a: left atrial disc, b: waist of device. A: anterior-posterior view of 32 mm ASO demonstrates the relationship of left atrial disc and waist size. B: anterior-posterior view of 12 mm ASO reveals that left atrial disc occupies large area in smaller device. ASO: Amplatzer septal occluder.

Fig. 2 The pathophysiologic mechanisms in elderly patients with atrial septal defect. Longstanding left to right shunt in the atrial level results in progressive right heart dilatation, significant TR and subsequent increase in RA pressure. Left heart may also be influenced by chronic volume underload, increased atrial pressure as well as co-morbid diseases. Lt: left, Rt: right, RAE: right atrial enlargement, RVE: right ventricular enlargement, LV: left ventricle, HTN: hypertension, IHD: ischemic heart disease, CO: cardiac output, PAH: pulmonary arterial hypertension, TR: tricuspid regurgitation, RAP: right atrial pressure, LAP: left atrial pressure, LAE: left atrial enlargement, A Fib: atrial fibrillation, A Flut: atrial flutter.

Fig. 3 Different protocols for the detection and management of high risk patients. If left ventricle restriction is detected, both protocols recommend several days of medical therapy including diuretics, inotropic agents and afterload reducing therapy, and if the patient is refractory to medical therapy on a subsequent balloon occlusion test, they recommend using a fenestrated device.5)14)15)23) LAP: left atrial pressure, ASD: atrial septal defect.
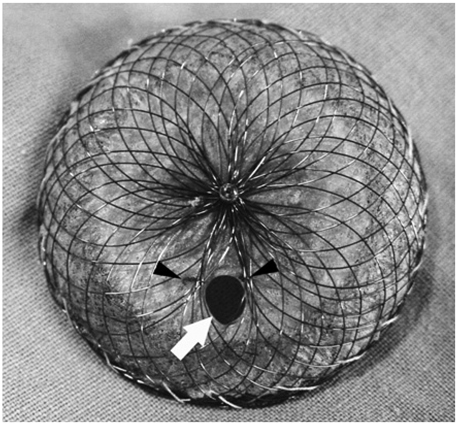
Fig. 4 Self-fabricated fenestrated device. Fabrication of the device by creating fenestration (white arrow) in both discs and connecting waist can be achieved using various sized dilators. Ties using non-absorbable suture materials (black arrow head) ensures the maintenance of fenestration.
Reference
-
1. Park MK. Pediatric Cardiology for Practitioners. 2008. 5th ed. Philadelphia: Mosby Elsevier;161–191.2. Bull C, Deanfield J, de Leval M, Stark J, Taylor JF, Macartney FJ. Correction of isolated secundum atrial septal defect in infancy. Arch Dis Child. 1981. 56:784–786.3. Lammers A, Hager A, Eicken A, Lange R, Hauser M, Hess J. Need for closure of secundum atrial septal defect in infancy. J Thorac Cardiovasc Surg. 2005. 129:1353–1357.4. Hijazi ZM, Celiker A. Closure of atrial septal defects. Anadolu Kardiyol Derg. 2005. 5:331.5. Holzer R, Hijazi ZM. Interventional approach to congenital heart disease. Curr Opin Cardiol. 2004. 19:84–90.6. Keane JF, Lock JE, Fyler DC. Nadas' Pediatric Cardiology. 2006. 2nd ed. Philadelphia: Saunders Elsevier;603–616.7. McMahon CJ, Feltes TF, Fraley JK, et al. Natural history of growth of secundum atrial septal defects and implications for transcatheter clo-sure. Heart. 2002. 87:256–259.8. Vogel M, Berger F, Dähnert I, Ewert P, Lange PE. Treatment of atrial septal defects in symptomatic children aged less than 2 years of age us-ing the Amplatzer septal occluder. Cardiol Young. 2000. 10:534–537.9. Diab KA, Cao QL, Bacha EA, Hijazi ZM. Device closure of atrial septal defects with the Amplatzer septal occluder: safety and outcome in infants. J Thorac Cardiovasc Surg. 2007. 134:960–966.10. Cardenas L, Panzer J, Boshoff D, Malekzadeh Milani S, Ovaert C. Transcatheter closure of secundum atrial defect in small children. Catheter Cardiovasc Interv. 2007. 69:447–452.11. Choi JY, Kim NK, Park SJ, Park HK, Park YH, Sul JH. Feasibility and safety of Transcatheter closure of atrial septal defect in small child-ren weighing 10kg or less. Catheter Cardiovasc Interv. 2008. 1:S10. Abstract.12. Wood AM, Holzer RJ, Texter KM, et al. Transcatheter elimination of left-to-right shunts in infants with bronchopulmonary dysplasia is feasible and safe. Congenit Heart Dis. 2011. 6:330–337.13. Amin Z. Transcatheter closure of secundum atrial septal defects. Catheter Cardiovasc Interv. 2006. 68:778–787.14. Spies C, Hijazi ZM. Transcatheter Closure of Secundum Atrial Septal Defects in the Elderly. Korean Circ J. 2009. 39:47–51.15. Schubert S, Peters B, Abdul-Khaliq H, Nagdyman N, Lange PE, Ewert P. Left ventricular conditioning in the elderly patient to prevent congestive heart failure after transcatheter closure of atrial septal defect. Catheter Cardiovasc Interv. 2005. 64:333–337.16. Swan L, Varma C, Yip J, et al. Transcatheter device closure of atrial septal defects in the elderly: technical considerations and short-term outcomes. Int J Cardiol. 2006. 107:207–210.17. Elshershari H, Cao QL, Hijazi ZM. Transcatheter device closure of atrial septal defects in patients older than 60 years of age: immediate and follow-up results. J Invasive Cardiol. 2008. 20:173–176.18. Shah D, Azhar M, Oakley CM, Cleland JG, Nihoyannopoulos P. Na-tural history of secundum atrial septal defect in adults after medical or surgical treatment: a historical prospective study. Br Heart J. 1994. 71:224–227.19. Attie F, Rosas M, Granados N, Zabal C, Buendía A, Calderón J. Surgical treatment for secundum atrial septal defects in patients >40 years old: a randomized clinical trial. J Am Coll Cardiol. 2001. 38:2035–2042.20. Miyaji K, Furuse A, Tanaka O, Kubota H, Ono M, Kawauchi M. Surgical repair for atrial septal defect in patients over 70 years of age. Jpn Heart J. 1997. 38:677–684.21. Shibata Y, Abe T, Kuribayashi R, et al. Surgical treatment of isolated secundum atrial septal defect in patients more than 50 years old. Ann Thorac Surg. 1996. 62:1096–1099.22. Yalonetsky S, Lorber A. Comparative changes of pulmonary artery pressure values and tricuspid valve regurgitation following transcatheter atrial septal defect closure in adults and the elderly. Congenit Heart Dis. 2009. 4:17–20.23. Ewert P, Berger F, Nagdyman N, et al. Masked left ventricular restriction in elderly patients with atrial septal defects: a contraindication for closure. Catheter Cardiovasc Interv. 2001. 52:177–180.24. Gatzoulis MA, Freeman MA, Siu SC, Webb GD, Harris L. Atrial arrhythmia after surgical closure of atrial septal defects in adults. N Engl J Med. 1999. 340:839–846.25. Oliver JM, Gallego P, Gonzlez A, Benito F, Mesa JM, Sobrino JA. Predisposing conditions for atrial fibrillation in atrial septal defect with and without operative closure. Am J Cardiol. 2002. 89:39–43.26. Silversides CK, Siu SC, McLaughlin PR, et al. Symptomatic atrial arrhythmias and transcatheter closure of atrial septal defects in adult patients. Heart. 2004. 90:1194–1198.27. Taniguchi M, Akagi T, Ohtsuki S, et al. Transcatheter closure of atrial septal defect in elderly patients with permanent atrial fibrillation. Catheter Cardiovasc Interv. 2009. 73:682–686.28. Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002. 347:1825–1833.29. Verma A, Natale A. Should atrial fibrillation ablation be considered first-line therapy for some patients? Why atrial fibrillation ablation should be considered first-line therapy for some patients. Circulation. 2005. 112:1214–1222.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comprehensive understanding of atrial septal defects by imaging studies for successful transcatheter closure
- Outcome of Transcatheter Closure of Oval Shaped Atrial Septal Defect with Amplatzer Septal Occluder
- Emergent Surgical Intervention for Embolization of Atrial Septal Defect Closure Device
- Transcatheter Closure of Secundum Atrial Septal Defect with the Amplatzer Septal Occluder
- Procedural, Early and Long-Term Outcomes after Transcatheter Atrial Septal Defects Closure: Comparison between Large and Very Large Atrial Septal Defect Groups
