Radiofrequency Catheter Ablation for Unifocal Premature Ventricular Complexes Triggering Recurrent Ventricular Fibrillations in a Young Man Without Structural Heart Disease
- Affiliations
-
- 1Cardiovascular Center, Dong-A University Hospital, Busan, Korea. thinkmed@dau.ac.kr
- KMID: 2225011
- DOI: http://doi.org/10.4070/kcj.2012.42.8.575
Abstract
- A 17-year-old man was referred for aborted sudden cardiac death. Ventricular fibrillation (VF) was recorded by automated external defibrillator. Post-resuscitation electrocardiograms showed frequent monomorphic premature ventricular complexes (PVCs), with left bundle branch block configuration and inferior axis. Cardiac arrest due to VF recurred twice within the initial 42 hours. Rhythm monitoring revealed multiple episodes of sustained VF triggered by a triplet of monomorphic PVCs having similar morphology with isolated PVCs. Comprehensive cardiologic workup revealed no structural heart disease and ion-channelopathies. With the impression of idiopathic VF triggered by unifocal PVCs of right ventricular outflow tract (RVOT) origin, radiofrequency catheter ablation was performed to prevent frequent VF recurrence before implantable cardioverter-defibrillator (ICD) implantation. After successful ablation of the origin of unifocal PVCs at anterolateral wall of RVOT, the burden of PVCs decreased remarkably and VF did not recur. The patient was discharged after ICD implantation.
MeSH Terms
Figure
-
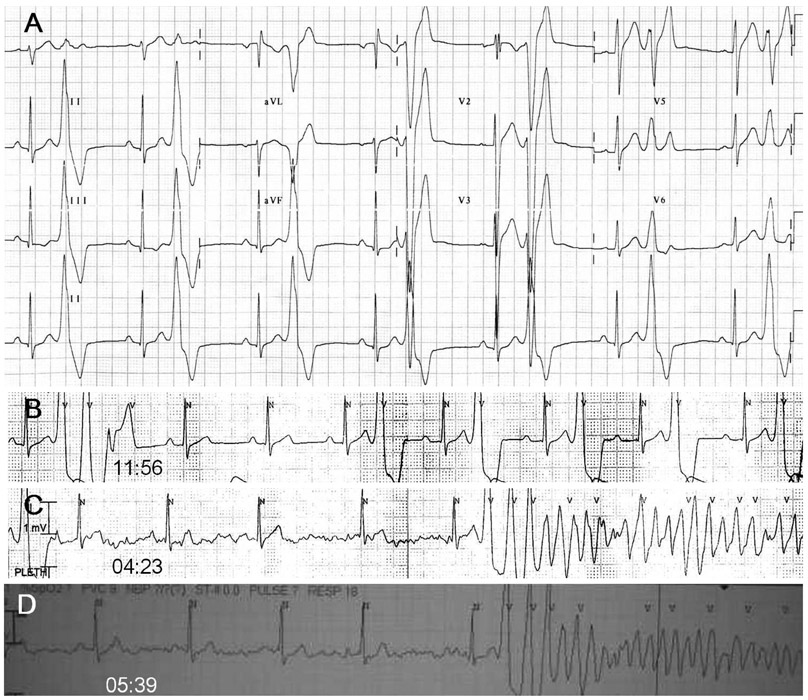
Fig. 1 Electrocardiographic characteristics of monomorphic PVCs and initiation of VF. A: post-resuscitation standard 12-lead ECG showed isolated monomorphic PVCs (coupling interval: 400 ms) with left bundle branch block configuration and inferior axis suggesting right ventricular outflow tract origin. B: rhythm recording 4 hours before the recurrence of VF showed frequent monomorphic PVCs with occasional couplets and triplets. C: rhythm recording at 04:23 showed an episode of fast polymorphic VT triggered by a triplet of monomorphic PVCs (coupling intervals: 360, 280, and 240 ms) having similar QRS morphology with isolated monomorphic PVCs. D: rhythm recording at 05:39 showed another episode of fast polymorphic VT triggered by a triplet of monomorphic PVCs with gradually shortened coupling intervals like prior episode (the picture was taken by a cellular phone camera). Induced fast polymorphic VT degenerated to sustained VF. PVC: premature ventricular complex, VF: ventricular fibrillation, ECG: electrocardiogram, VT: ventricular tachycardia.
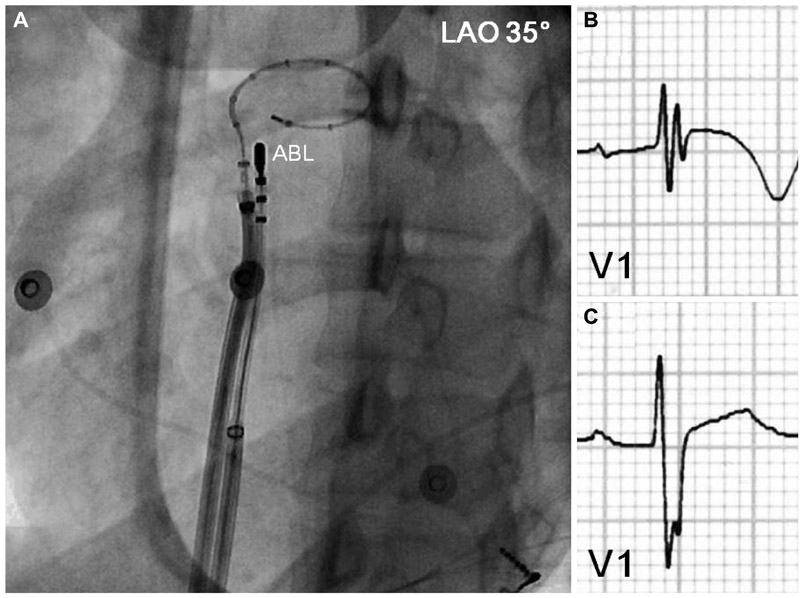
Fig. 2 Intracardiac mapping for monomorphic PVCs of RVOT origin. A: a deflectable ablation catheter and a 20-pole variable circular mapping catheter were placed at RVOT using long guiding sheathes. The circular mapping catheter with 25 mm diameter was positioned at 1 cm below pulmonary valve. The tip of ablation catheter was positioned at anterolateral wall of RVOT 2 cm below pulmonary valve, where the earliest ventricular activation signal was recorded during activation mapping for spontaneous PVCs. B: ECG before radiofrequency catheter ablation showed fragmented QRS complex with T wave inversion in V1. C: however, the fragmentation of QRS complex and T wave inversion disappeared after successful ablation. PVC: premature ventricular complex, RVOT: right ventricular outflow tract, ABL: ablation catheter, LAO: left anterior oblique view, ECG: eletrocardiogram.
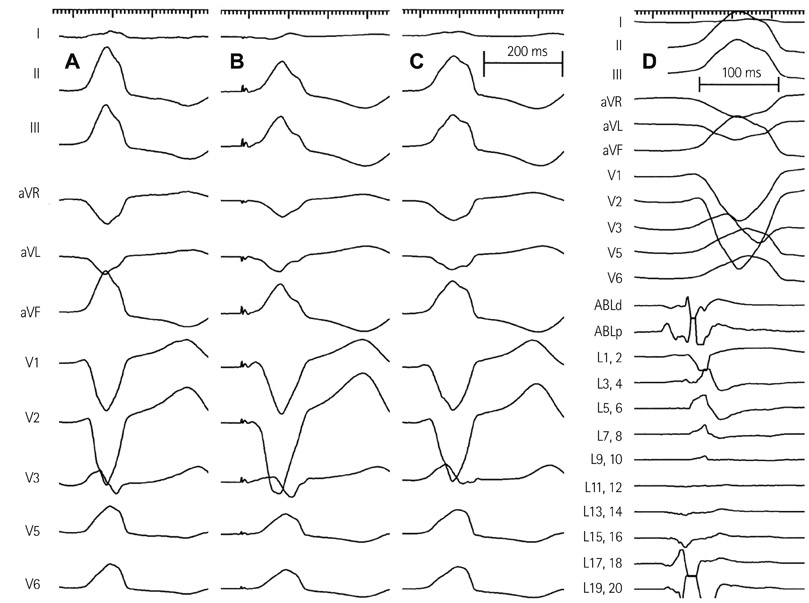
Fig. 3 Activation and paced mapping for radiofrequency catheter ablation. A: spontaneous PVCs during electrophysiologic study had left bundle branch block configuration and inferior axis. B: paced mapping at anterolateral wall of RVOT 2 cm below pulmonary valve showed the QRS morphology nearly identical with spontaneous PVCs. C: the morphology of accelerated ventricular rhythm induced by radiofrequency ablation also had the QRS morphology nearly identical with spontaneous PVCs. D: activation mapping for spontaneous PVCs showed the earliest ventricular activation signal 20 ms prior to the QRS onset. PVC: premature ventricular complex, RVOT: right ventricular outflow tract, ABLd: distal ablation catheter, ABLp: proximal ablation catheter, L: Lasso variable circular mapping catheter.
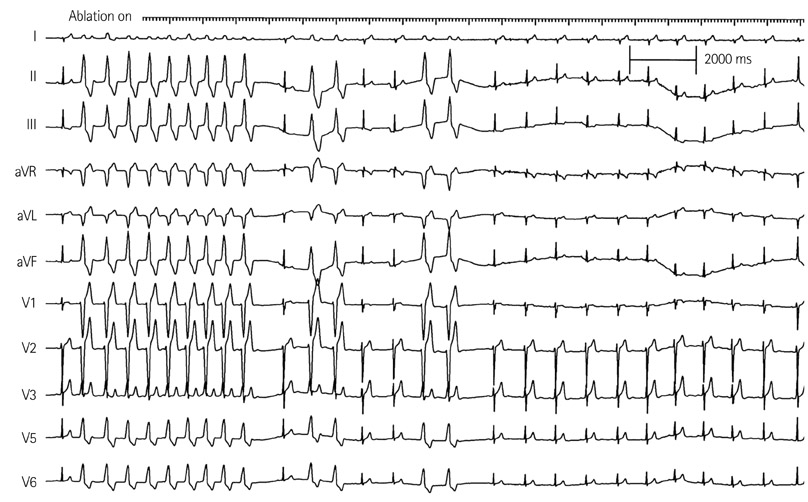
Fig. 4 Radiofrequency ablation and disappearance of monomorphic PVCs. Accelerated ventricular rhythm having the QRS morphology nearly identical with spontaneous PVCs was induced transiently after starting radiofrequency ablation. Induced accelerated ventricular rhythm and frequent monomorphic PVCs disappeared in 12 seconds during ongoing radiofrequency ablation. PVC: premature ventricular complex.
Cited by 1 articles
-
Cardiac Arrest due to Recurrent Ventricular Fibrillation Triggered by Unifocal Ventricular Premature Complexes in a Silent Myocardial Infarction
Dong Hyun Lee, Seul Lee, Hyo Jin Jung, Soo Jin Kim, Jeong-Min Seo, Jae-Hyuk Choi, Jong Sung Park
Korean J Crit Care Med. 2014;29(4):331-335. doi: 10.4266/kjccm.2014.29.4.331.
Reference
-
1. Survivors of out-of-hospital cardiac arrest with apparently normal heart: need for definition and standardized clinical evaluation: consensus Statement of the Joint Steering Committees of the Unexplained Cardiac Arrest Registry of Europe and of the Idiopathic Ventricular Fibrillation Registry of the United States. Circulation. 1997. 95:265–272.2. Haïssaguerre M, Shoda M, Jaïs P, et al. Mapping and ablation of idiopathic ventricular fibrillation. Circulation. 2002. 106:962–967.3. Uemura T, Yamabe H, Tanaka Y, et al. Catheter ablation of a polymorphic ventricular tachycardia inducing monofocal premature ventricular complex. Intern Med. 2008. 47:1799–1802.4. Nogami A, Sugiyasu A, Kubota S, Kato K. Mapping and ablation of idiopathic ventricular fibrillation from the Purkinje system. Heart Rhythm. 2005. 2:646–649.5. Buxton AE, Waxman HL, Marchlinski FE, Simson MB, Cassidy D, Josephson ME. Right ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation. 1983. 68:917–927.6. Noda T, Shimizu W, Taguchi A, et al. Malignant entity of idiopathic ventricular fibrillation and polymorphic ventricular tachycardia initiated by premature extrasystoles originating from the right ventricular outflow tract. J Am Coll Cardiol. 2005. 46:1288–1294.7. Knecht S, Sacher F, Wright M, et al. Long-term follow-up of idiopathic ventricular fibrillation ablation: a multicenter study. J Am Coll Cardiol. 2009. 54:522–528.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiofrequency Ablation of Recurrent Ventricular Premature Complex Originating from near Left Ventricular Summit Guided by Intracardiac Echocardiography
- Catheter Ablation for Brugada Syndrome
- Catheter Ablation of Parahisian Premature Ventricular Complex
- Radiofrequency Catheter Ablation of Ventricular Tachycardia in Patients without Structural Heart Disease
- Tachycardiomyopathy Induced by Ventricular Premature Complexes: Complete Recovery after Radiofrequency Catheter Ablation
