Catheter Ablation for Brugada Syndrome
- Affiliations
-
- 1Department of Cardiology, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan. anogami@md.tsukuba.ac.jp
- 2Division of Cardiac Electrophysiology, Al Najaf Center for Cardiac Surgery and Trans-Catheter Therapy, Najaf, Iraq.
- KMID: 2471279
- DOI: http://doi.org/10.4070/kcj.2019.0344
Abstract
- Brugada syndrome (BrS) is an arrhythmogenic disease associated with an increased risk of ventricular fibrillation (VF) and sudden cardiac death (SCD). To date, the standard therapy for the prevention of SCD in BrS is the use of an implantable cardioverter-defibrillator (ICD) especially in patients who have experienced a prior cardiac arrest or syncopal events secondary to VF. However, ICDs do not prevent the occurrence of VF but react to defibrillate the VF episode, thereby preventing SCD. Often patients with recurrent VF have to be maintained on antiarrhythmic drugs that are effective but have remarkable adverse effects. An alternative therapy for BrS with recurrent VF is catheter ablation which emerged as an effective therapy in eliminating VF-triggering premature ventricular complexes in limited case series; however, there has been a remarkable progress in effectiveness of catheter ablation since epicardial substrate ablation was first applied in 2011 and such approach is now widely applicable.
MeSH Terms
Figure
-
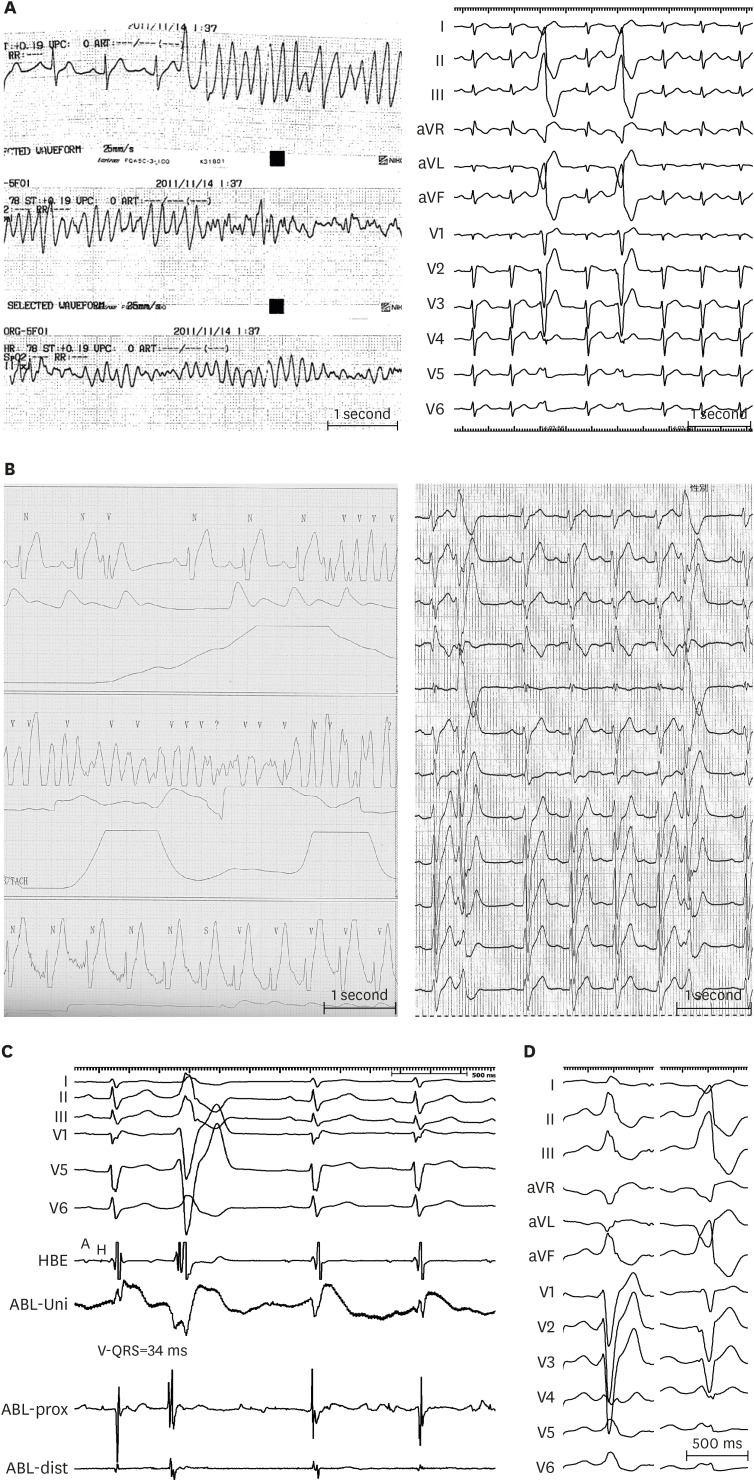
Figure 1 (A) Serial ECG strips of a BrS patient presented to the emergency room after resuscitation from VF. Frequent monofocal PVCs reproducibly degenerated into VF, leading to electrical storm. PVCs exhibited LBBB and inferior axis morphology. (B) Telemetry of a BrS patient presented with recurrent VF episodes. 12-lead ECG taken immediately after implantable cardioverter-defibrillator discharge showed PVCs with LBBB and superior axis configuration. (C) Intracardiac recordings at a successful ablation site of a VF-triggering PVC. The local ventricular activation recorded by the distal electrode pair of the ABL preceded the QRS complex onset by 34 ms with QS configuration of the unipolar electrogram. (D) VF-triggering PVC immediately after electrical storm (right) of a young male who underwent emergency VF-trigger ablation. Culprit PVC exhibits LBBB pattern and inferior axis. After culprit PVC elimination, VF became non-inducible after electrophysiology study with triple RV extra-stimuli. Pilsicainide infusion could induce a PVC of LBBB pattern, inferior axis indicating RV outflow tract origin (right); however the induced PVC morphology was different from VF-triggering PVC and was not ablated. The patient has been VF-free for 8-year follow-up.Modified from Talib AK, et al. Efficacy of endocardial ablation of drug-resistant ventricular fibrillation in Brugada syndrome: long-term outcome. Circ Arrhythm Electrophysiol 2018;11:e006675.15)A = atrial potential; ABL = ablation catheter; aVF = augmented vector foot; aVL = augmented vector left; aVR = augmented vector right; BrS = Brugada syndrome; dist = distal bipole; ECG = electrocardiogram; H = his potential; HBE = his bundle electrogram; LBBB = left bundle-branch block; prox = proximal; PVC = premature ventricular complex; RV = right ventricular; Uni = unipolar electrogram; VF = ventricular fibrillation.
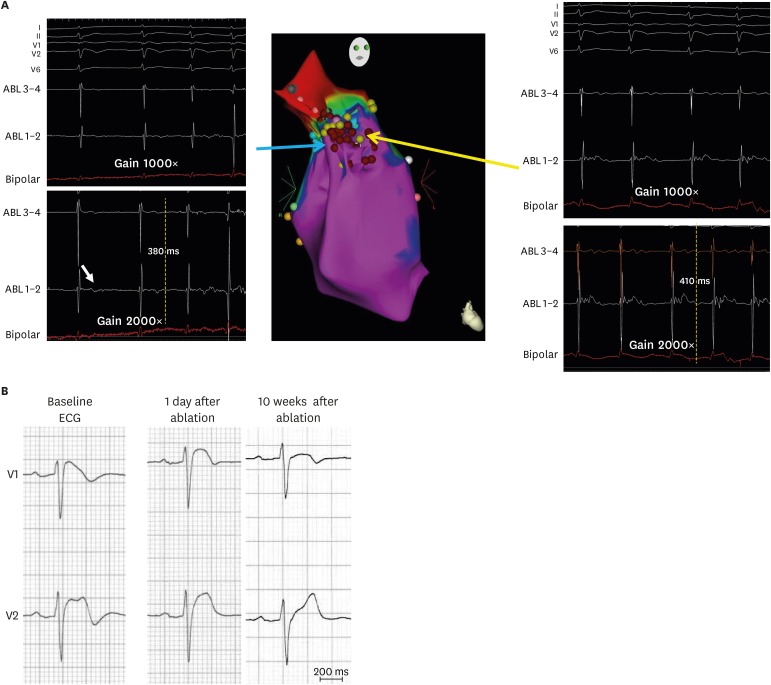
Figure 2 (A) Right anterior oblique view of 3-dimensional electroanatomical mapping of endocardial aspect of the RVOT where delayed low voltage fractionated EGMs were found at the RVOT lateral wall (red tags represent ablation points). Note these low voltage EGMs could be revealed using larger than the standard gain (2,000×) (B) Right precordial ECGs of a Brugada syndrome patient showing normalization of Brugada-type ST-segment elevation 10 weeks after endocardial ablation.Modified from Talib AK, et al. Efficacy of endocardial ablation of drug-resistant ventricular fibrillation in Brugada syndrome: long-term outcome. Circ Arrhythm Electrophysiol 2018;11:e006675.15)ABL = ablation catheter; ECG = electrocardiogram; EGM = electrogram; RVOT = right ventricular outflow tract.
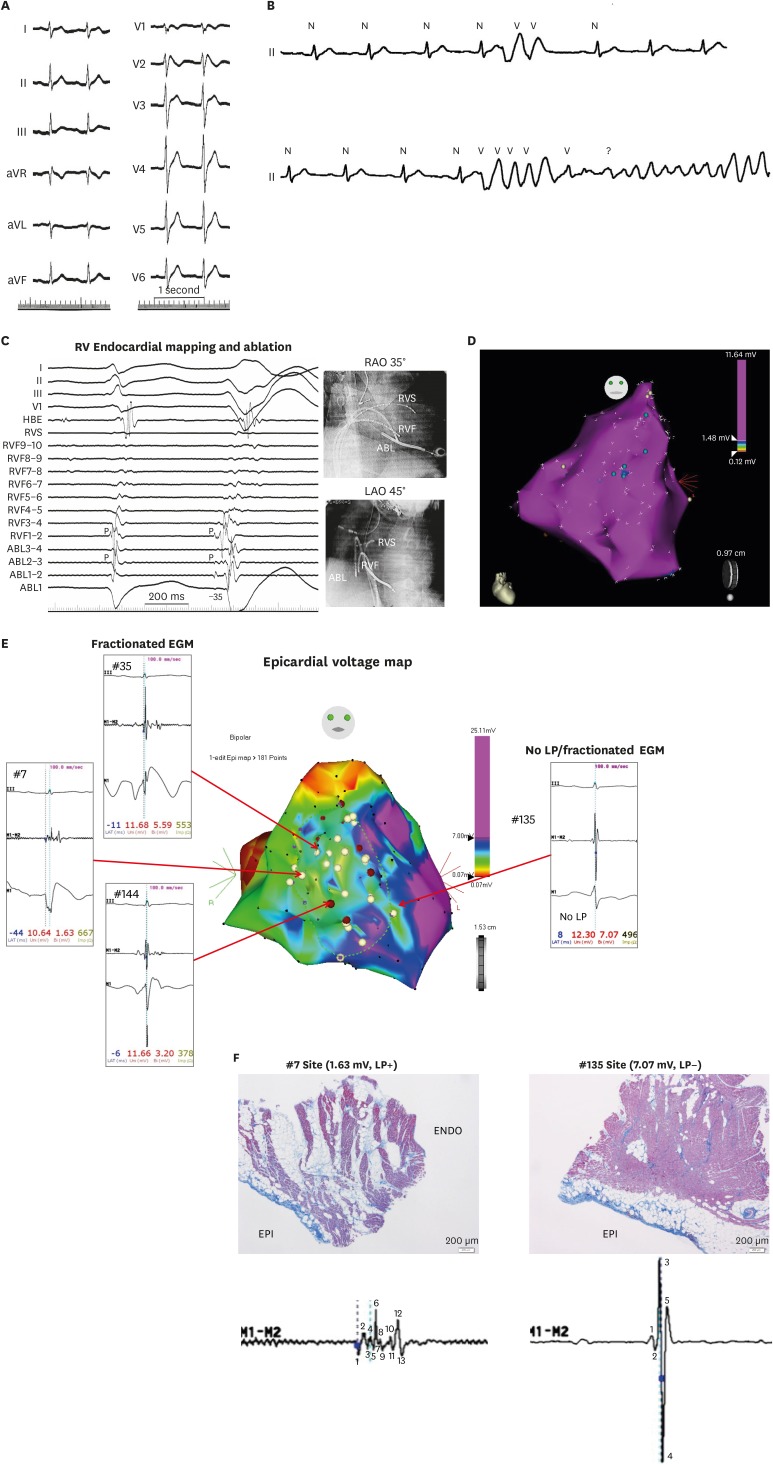
Figure 3 (A) A 12–lead electrocardiogram of a 27-year-old male with Brugada syndrome and SCN5A mutation Note QRS notching in lead V1. (B) After Pilsicainide infusion, Frequent PVCs were observed which degenerated into VF. (C) Mapping showed the earliest activation of the VF-triggering PVCs were observed at the RVF where presystolic Purkinje potential preceding the QRS onset of the PVC by 35 ms. Note that Purkinje potential is observed locally during sinus rhythm. (D) Endocardial electroanatomical mapping, repeated 8 years after the initial endocardial session, revealed normal RV/RV outflow tract voltage and confirmed elimination of previously ablated endocardial EGMs. Blue tags indicate remnant previously ablated LP. (E) Intraoperative epicardial mapping revealed relatively low voltage area with fractionated EGMs at the epicardial surface of previously ablated endocardial EGMs. Interestingly, coved-type ST-segment elevation was observed in the unipolar recordings of the ablation catheter at the fractionated EGM areas. (F) Epicardial biopsy and histology shows epicardial fibrosis with focal finger-like projections of collagen into myocardium while EGM-free areas revealed neither abnormal potential nor myocardial fibrosis.Modified from Talib AK, et al. Efficacy of endocardial ablation of drug-resistant ventricular fibrillation in Brugada syndrome: long-term outcome. Circ Arrhythm Electrophysiol 2018;11:e006675.15)ABL = ablation catheter; aVF = augmented vector foot; aVL = augmented vector left; aVR = augmented vector right; EGM = electrogram; HBE = his bundle electrogram; LAO = left anterior oblique; LP = late potentials; PVC = premature ventricular complex; RAO = right anterior oblique; RVF = RV free wall; RV = right ventricular; RVS = RV septum; VF = ventricular fibrillation.
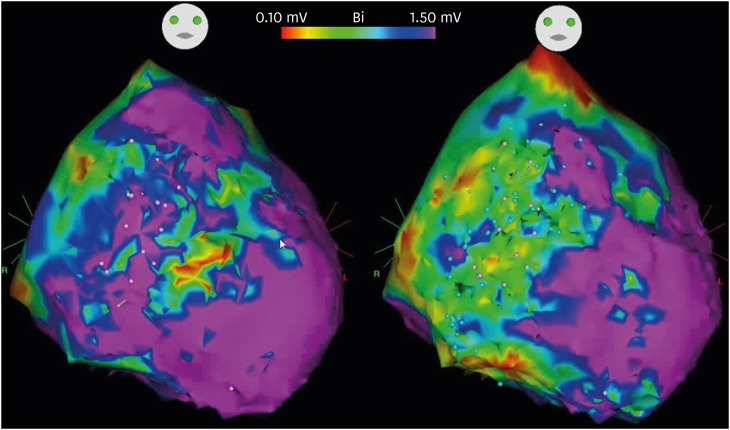
Figure 4 Electro-anatomical map of epicardial substrate of a 22-year-old male with Brugada syndrome. Baseline voltage map showed low voltage areas at the anterior and lateral aspects and RV and RVOT (left). After Pilsicainide infusion, the low voltage areas extended to involve almost the entire anterior and lateral aspects of RV and RVOT (right).RV = right ventricular; RVOT = right ventricular outflow tract.
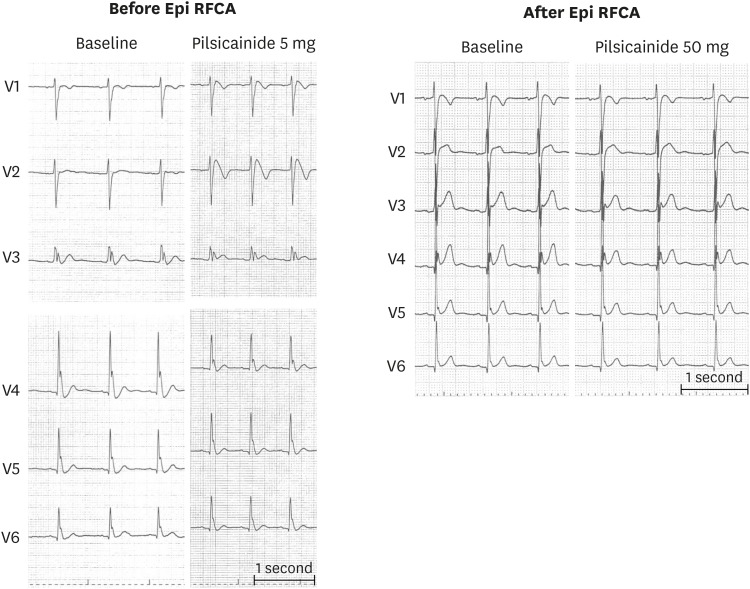
Figure 5 A 12-lead ECG of a young male who presented with electrical storm. Baseline ECG showed J-wave in leads V3–V6 and after very low dose (5 mg) Pilsicainide infusion, coved type ECG pattern was observed resulting in global type early repolarization (left). Despite extensive epicardial ablation at the RV/RV outflow tract with sodium channel blockade guide, Brugada ECG pattern could be eliminated even after higher dose Pilsicainide however, lateral chest lead J-wave could not be eliminated (right). Such patients may remain at high-risk of developing VF after ablation.ECG = electrocardiogram; RFCA = radiofrequency catheter ablation; RV = right ventricular; VF = ventricular fibrillation.
Cited by 1 articles
-
Can Artemisinin Be a Game Changer Even as an Antiarrhythmic Drug?
Jongmin Hwang
Korean Circ J. 2023;53(4):251-253. doi: 10.4070/kcj.2023.0031.
Reference
-
1. Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol. 1992; 20:1391–1396. PMID: 1309182.2. Hermida JS, Lemoine JL, Aoun FB, Jarry G, Rey JL, Quiret JC. Prevalence of the Brugada syndrome in an apparently healthy population. Am J Cardiol. 2000; 86:91–94. PMID: 10867101.3. Furuhashi M, Uno K, Tsuchihashi K, et al. Prevalence of asymptomatic ST segment elevation in right precordial leads with right bundle branch block (Brugada-type ST shift) among the general Japanese population. Heart. 2001; 86:161–166. PMID: 11454832.4. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2015; 36:2793–2867. PMID: 26320108.5. Belhassen B, Glick A, Viskin S. Efficacy of quinidine in high-risk patients with Brugada syndrome. Circulation. 2004; 110:1731–1737. PMID: 15381640.6. Viskin S, Wilde AA, Guevara-Valdivia ME, et al. Quinidine, a life-saving medication for Brugada syndrome, is inaccessible in many countries. J Am Coll Cardiol. 2013; 61:2383–2387. PMID: 23583244.7. Haïssaguerre M, Extramiana F, Hocini M, et al. Mapping and ablation of ventricular fibrillation associated with long-QT and Brugada syndromes. Circulation. 2003; 108:925–928. PMID: 12925452.8. Nademanee K, Veerakul G, Chandanamattha P, et al. Prevention of ventricular fibrillation episodes in Brugada syndrome by catheter ablation over the anterior right ventricular outflow tract epicardium. Circulation. 2011; 123:1270–1279. PMID: 21403098.9. Kakishita M, Kurita T, Matsuo K, et al. Mode of onset of ventricular fibrillation in patients with Brugada syndrome detected by implantable cardioverter defibrillator therapy. J Am Coll Cardiol. 2000; 36:1646–1653. PMID: 11079671.10. Morita H, Fukushima-Kusano K, Nagase S, et al. Site-specific arrhythmogenesis in patients with Brugada syndrome. J Cardiovasc Electrophysiol. 2003; 14:373–379. PMID: 12741708.11. Nademanee K, Raju H, de Noronha SV, et al. Fibrosis, connexin-43, and conduction abnormalities in the Brugada syndrome. J Am Coll Cardiol. 2015; 66:1976–1986. PMID: 26516000.12. Coronel R, Casini S, Koopmann TT, et al. Right ventricular fibrosis and conduction delay in a patient with clinical signs of Brugada syndrome: a combined electrophysiological, genetic, histopathologic, and computational study. Circulation. 2005; 112:2769–2777. PMID: 16267250.13. Darmon JP, Bettouche S, Deswardt P, et al. Radiofrequency ablation of ventricular fibrillation and multiple right and left atrial tachycardia in a patient with Brugada syndrome. J Interv Card Electrophysiol. 2004; 11:205–209. PMID: 15548887.14. Nakagawa E, Takagi M, Tatsumi H, Yoshiyama M. Successful radiofrequency catheter ablation for electrical storm of ventricular fibrillation in a patient with Brugada syndrome. Circ J. 2008; 72:1025–1029. PMID: 18503235.15. Talib AK, Takagi M, Shimane A, et al. Efficacy of endocardial ablation of drug-resistant ventricular fibrillation in Brugada syndrome: long-term outcome. Circ Arrhythm Electrophysiol. 2018; 11:e006675. PMID: 30354324.16. Krittayaphong R, Veerakul G, Nademanee K, Kangkagate C. Heart rate variability in patients with Brugada syndrome in Thailand. Eur Heart J. 2003; 24:1771–1778. PMID: 14522573.17. Talib AK, Yui Y, Kaneshiro T, Sekiguchi Y, Nogami A, Aonuma K. Alternative approach for management of an electrical storm in Brugada syndrome: importance of primary ablation within a narrow time window. J Arrhythm. 2016; 32:220–222. PMID: 27354869.18. Shah AJ, Hocini M, Lamaison D, Sacher F, Derval N, Haissaguerre M. Regional substrate ablation abolishes Brugada syndrome. J Cardiovasc Electrophysiol. 2011; 22:1290–1291. PMID: 21457386.19. Sunsaneewitayakul B, Yao Y, Thamaree S, Zhang S. Endocardial mapping and catheter ablation for ventricular fibrillation prevention in Brugada syndrome. J Cardiovasc Electrophysiol. 2012; 23(Suppl 1):S10–S16. PMID: 22988965.20. Hayashi T, Nitta J, Goya M, Isobe M, Hirao K. Endocardial-only catheter ablation with substantial improvement in ventricular fibrillation recurrences in a patient with Brugada syndrome. HeartRhythm Case Rep. 2016; 2:428–431. PMID: 28491726.21. Morita H, Zipes DP, Morita ST, Lopshire JC, Wu J. Epicardial ablation eliminates ventricular arrhythmias in an experimental model of Brugada syndrome. Heart Rhythm. 2009; 6:665–671. PMID: 19328041.22. Brugada J, Pappone C, Berruezo A, et al. Brugada syndrome phenotype elimination by epicardial substrate ablation. Circ Arrhythm Electrophysiol. 2015; 8:1373–1381. PMID: 26291334.23. Pappone C, Brugada J, Vicedomini G, et al. Electrical substrate elimination in 135 consecutive patients with Brugada syndrome. Circ Arrhythm Electrophysiol. 2017; 10:e005053. PMID: 28500178.24. Sacher F, Jesel L, Jais P, Haïssaguerre M. Insight into the mechanism of Brugada syndrome: epicardial substrate and modification during ajmaline testing. Heart Rhythm. 2014; 11:732–734. PMID: 23732228.25. Chung FP, Raharjo SB, Lin YJ, et al. A novel method to enhance phenotype, epicardial functional substrates, and ventricular tachyarrhythmias in Brugada syndrome. Heart Rhythm. 2017; 14:508–517. PMID: 28065832.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Idiopathic Brugada ECG Pattern Developed in Relation To Fever
- Large Circular Ring Catheter Ablation Versus Anatomically Guided Ablation of Atrial Fibrillation: Back to the Future for Successful Catheter Ablation of Atrial Fibrillation?
- Anesthesia in a Patient with Brugada Syndrome without a Characteristic ECG Pattern: A case report
- COVID-19 Vaccination-Induced Ventricular Fibrillation in an Afebrile Patient With Brugada Syndrome
- Brugada Syndrome Presenting With Convulsion in the Emergency Department: A Case Report
