A Case of Abdominal Aortic Aneurysm with Short Angulated Proximal Neck Treated with the Chimney Graft Technique
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea. ygko@yuhs.ac
- 2Department of Radiology, Severance Hospital, Yonsei University Health System, Seoul, Korea.
- KMID: 2224904
- DOI: http://doi.org/10.4070/kcj.2013.43.6.416
Abstract
- Endovascular aneurysm repair (EVAR) using stent grafts has shown to be an effective alternative to surgical repair in treating an abdominal aortic aneurysm (AAA). EVAR is associated with shorter hospital stays, less blood loss, shorter operating times, and lower early morbidity and mortality compared to open surgical repair, although EVAR required a higher reintervention rate during a longer follow-up period. However, short or severely an angulated infrarenal proximal aortic neck is considered unsuitable for EVAR. The chimney graft technique is a modified procedure based on the deployment of a covered or bare-metal stent parallel to the main aortic endograft within the aneurysm, thereby creating a conduit that runs outside the aortic main endograft to preserve flow to the aortic branches. In this case report, we present a 78-year-old patient with an AAA with a short and severely angulated proximal neck who was successfully treated by EVAR using the chimney graft technique.
MeSH Terms
Figure
-
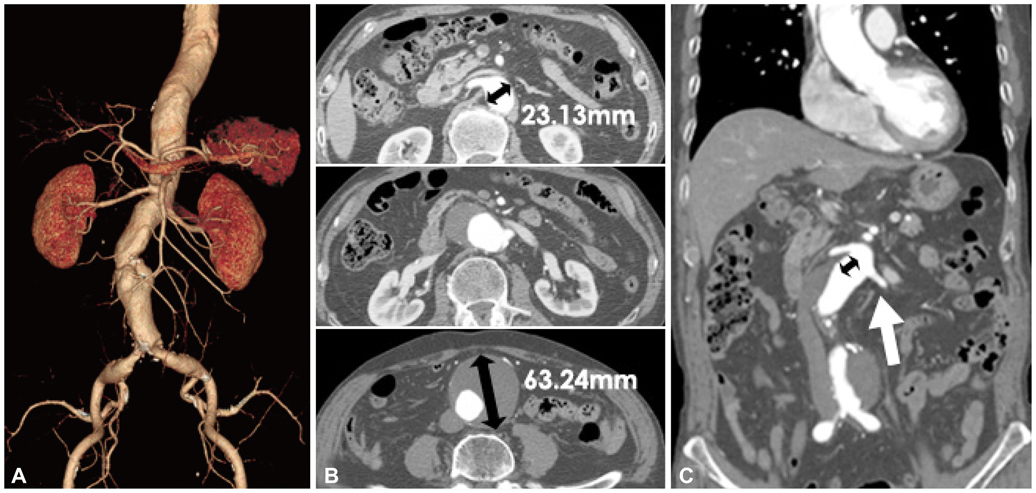
Fig. 1 Baseline CT images of abdominal aortic aneurysm. A: three dimensional reconstruction image of the abdominal aortic aneurysm. B: axial view of abdominal aortic aneurysm at right renal artery (upper) and left renal artery level (middle) with a maximum diameter of 63 mm (below). C: coronal view of the infrarenal abdominal aortic artery, the black arrow indicates the length of the aortic neck to the right renal artery orifice which was 16 mm, and the white arrow indicates the left renal artery. The left renal artery orifice was adjacent to the aneurysm and there was practically no neck.
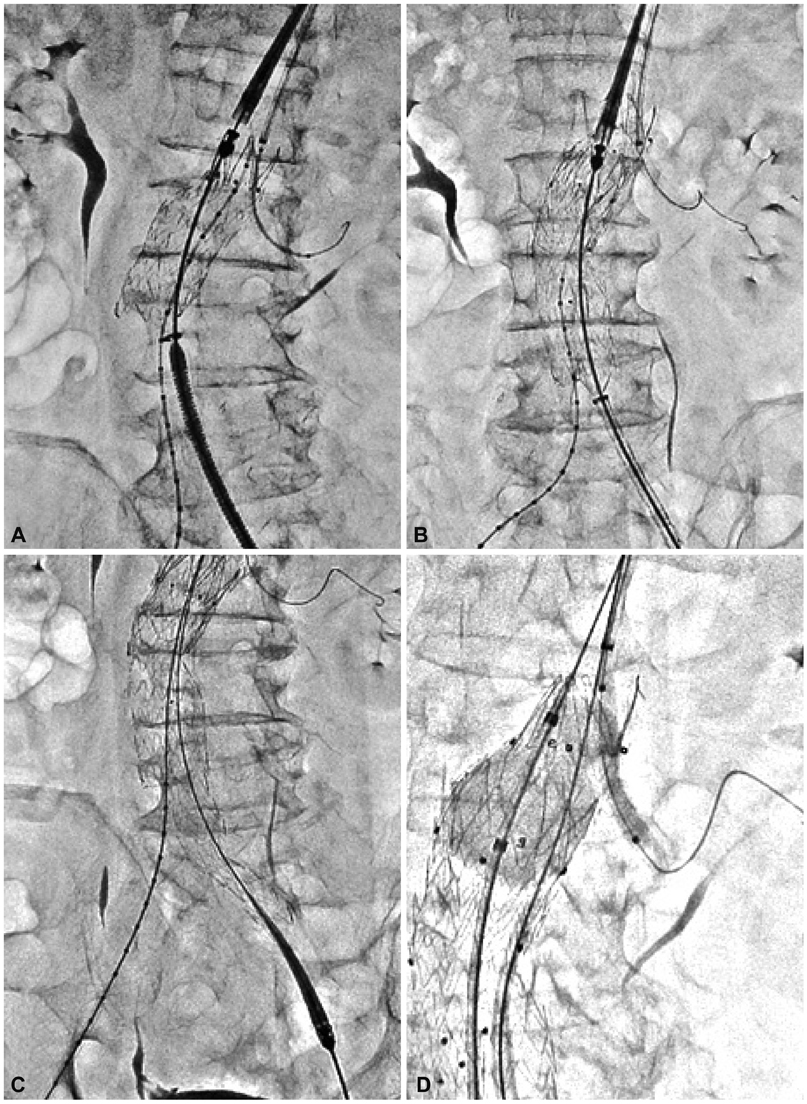
Fig. 2 Procedure steps of the chimney technique. A: insertion of an aortic extension stent graft (36×70 mm, Endurant, Medtronic, Santa Rosa, CA, USA) and a renal stent graft (6×50 mm, Viabahn, Gore, Flagshiff, AR, USA). B: the main body (36×20×166 mm, Endurant, Medtronic) was inserted at AAA in overlapping with the distal part of the aortic extension stent graft. C: adjuvant balloon dilation was performed by kissing balloon technique using a 46 mm Reliant balloon (Medtronic) for aorta stent graft and a 6×40 mm balloon for the left renal stent graft. D: additional balloon dilation of bifurcated stent graft was performed.

Fig. 3 Angiographic result after endovascular aneurysm repair using the Chimney graft technique. A: final angiogram showing no significant endoleak and patent left renal artery. B: stent at main body and left artery. C: flow through the left renal artery.

Fig. 4 A CT scan taken 4 days after the procedure showing complete exclusion of the abdominal aortic aneurysm sac and patent Viabahn stent graft deployed in the left renal artery. A: 3 dimensional reconstruction view. B: axial view of the aortic stent. White arrows indicate the stent graft in the left renal artery.
Reference
-
1. Schermerhorn ML, O'Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008; 358:464–474.2. Brewster DC, Cronenwett JL, Hallett JW Jr, et al. Guidelines for the treatment of abdominal aortic aneurysms. Report of a subcommittee of the Joint Council of the American Association for Vascular Surgery and Society for Vascular Surgery. J Vasc Surg. 2003; 37:1106–1117.3. Lindsay TF. Canadian Society for Vascular Surgery. Canadian Society for Vascular Surgery consensus statement on endovascular aneurysm repair. CMAJ. 2005; 172:867–868.4. Ernst CB. Abdominal aortic aneurysm. N Engl J Med. 1993; 328:1167–1172.5. Hertzer NR, Mascha EJ, Karafa MT, O'Hara PJ, Krajewski LP, Beven EG. Open infrarenal abdominal aortic aneurysm repair: the Cleveland Clinic experience from 1989 to 1998. J Vasc Surg. 2002; 35:1145–1154.6. EVAR trial participants. Endovascular aneurysm repair and outcome in patients unfit for open repair of abdominal aortic aneurysm (EVAR trial 2): randomised controlled trial. Lancet. 2005; 365:2187–2192.7. Greenberg R, Fairman R, Srivastava S, Criado F, Green R. Endovascular grafting in patients with short proximal necks: an analysis of short-term results. Cardiovasc Surg. 2000; 8:350–354.8. Greenberg RK, Clair D, Srivastava S, et al. Should patients with challenging anatomy be offered endovascular aneurysm repair? J Vasc Surg. 2003; 38:990–996.9. Stanley BM, Semmens JB, Mai Q, et al. Evaluation of patient selection guidelines for endoluminal AAA repair with the Zenith Stent-Graft: the Australasian experience. J Endovasc Ther. 2001; 8:457–464.10. Leurs LJ, Kievit J, Dagnelie PC, Nelemans PJ, Buth J. EUROSTAR Collaborators. Influence of infrarenal neck length on outcome of endovascular abdominal aortic aneurysm repair. J Endovasc Ther. 2006; 13:640–648.11. Donas KP, Pecoraro F, Torsello G, et al. Use of covered chimney stents for pararenal aortic pathologies is safe and feasible with excellent patency and low incidence of endoleaks. J Vasc Surg. 2012; 55:659–665.12. Moulakakis KG, Mylonas SN, Avgerinos E, et al. The chimney graft technique for preserving visceral vessels during endovascular treatment of aortic pathologies. J Vasc Surg. 2012; 55:1497–1503.13. Ohrlander T, Sonesson B, Ivancev K, Resch T, Dias N, Malina M. The chimney graft: a technique for preserving or rescuing aortic branch vessels in stent-graft sealing zones. J Endovasc Ther. 2008; 15:427–432.14. Greenberg RK, Sternbergh WC 3rd, Makaroun M, et al. Intermediate results of a United States multicenter trial of fenestrated endograft repair for juxtarenal abdominal aortic aneurysms. J Vasc Surg. 2009; 50:730–737.e1.15. Panuccio G, Greenberg RK, Wunderle K, Mastracci TM, Eagleton MG, Davros W. Comparison of indirect radiation dose estimates with directly measured radiation dose for patients and operators during complex endovascular procedures. J Vasc Surg. 2011; 53:885–894.e1. discussion 894.16. Hiramoto JS, Chang CK, Reilly LM, Schneider DB, Rapp JH, Chuter TA. Outcome of renal stenting for renal artery coverage during endovascular aortic aneurysm repair. J Vasc Surg. 2009; 49:1100–1106.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Repair of a Juxtarenal Abdominal Aortic Aneurysm Using a Chimney Graft
- Repair of type I endoleak by chimney technique after endovascular abdominal aortic aneurysm repair
- Thrombotic Occlusion of Stent Graft Limbs due to Severe Angulation of Aortic Neck in Endovascular Repair of Abdominal Aortic Aneurysm
- The Modified Chimney Technique With a Thoracic Aortic Stent Graft to Preserve the Blood Flow of the Left Common Carotid Artery for Treating Descending Thoracic Aortic Aneurysm and Dissection
- Total Endovascular Therapy of Abdominal Aortic Aneurysm, Peripheral Artery Disease, and Chronic Mesenteric Ischemia: A Challenging Case
