Familial Hypercholesterolemia and the Atherosclerotic Disease
- Affiliations
-
- 1Department of Cardiology, College of Medicine, University of Ulsan, Asan Medical Center, Seoul, Korea. steadyhan@amc.seoul.kr
- KMID: 2224895
- DOI: http://doi.org/10.4070/kcj.2013.43.6.363
Abstract
- Familial hypercholesterolemia (FH) is associated with premature atherosclerotic cardiovascular diseases, and is inherited as an autosomal dominant trait. The prevalence of heterozygous FH is one in five hundred people. Owing to dysfunctional low density lipoprotein (LDL) receptors due to genetic mutations, serum low density lipoprotein-cholesterol (LDL-C) levels are considerably increased from birth. FH is clinically diagnosed by confirmation of family history and characteristic findings such as tendon xanthoma or xanthelasma. Thus, clinical concern and suspicion are important for early diagnosis of the disease. Current guidelines recommend lowering LDL-C concentration to at least 50% from baseline. Statins are shown to lower LDL-C levels with high safety, and thus, have been the drug of choice. However, it is difficult to achieve an ideal level of LDL-C with a single statin therapy in the majority of FH patients. Alternatively, lipid lowering combination therapy with the recently-introduced ezetimibe has shown more encouraging results.
Keyword
MeSH Terms
Figure
-
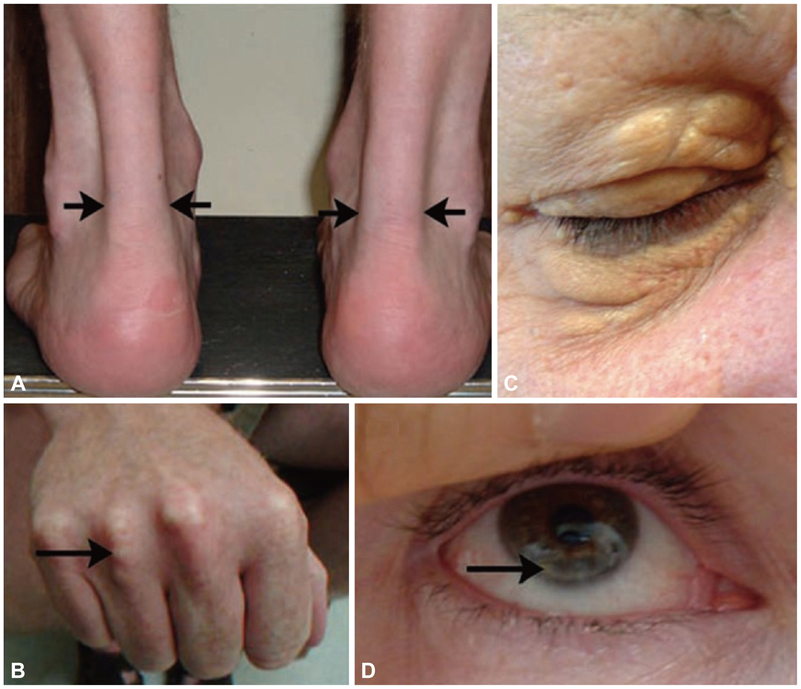
Fig. 1 Physical signs of heterozygous familial hypercholesterolemia, as a result of cholesterol deposition within macrophages in specific sites. Tendinous xanthomas, for example, manifests first as thickening of, and later as deposits within, extensor tendons. A: lateral borders of thickened Achilles' tendons are shown with arrows. B: tendinous xanthomas can also occur in the extensor tendons of the hands (shown), feet, elbows and knees. C: xanthelasmas are cholesterol deposits in the eyelids. D: arcus cornealis results from cholesterol infiltration around the corneal rim (arrow) (Yuan G, Wang J, Hegele RA. CMAJ 2006;174:1124-9).9)

Fig. 2 The role of PCSK9 proteins. PCSK9 genes are synthesized in the golgi complex and secreted into the blood. These genes combine with LDL receptors and go through lysosomal degradation. The assumption is that there is a mechanism in which LDL receptors, which underwent endocytosis, are degraded in the Golgi bodies (Akram ON, Bernier A, Petrides F, Wong G, Lambert G. Arterioscler Thromb Vasc Biol 2010;30:1279-81). LDL: low density lipoprotein.15)
Reference
-
1. Wierzbicki AS, Humphries SE, Minhas R. Guideline Development Group. Familial hypercholesterolaemia: summary of NICE guidance. BMJ. 2008; 337:a1095.2. World Health Organization Human Genetics Programme. Familial Hypercholesterolaemia (FH): Report of a Second WHO Consultation, Geneva, 4 September 1998. Geneva: World Health Organization, Human Genetics Program;1999.3. Scientific Steering Committee on behalf of the Simon Broome Register Group. Risk of fatal coronary heart disease in familial hypercholesterolaemia. BMJ. 1991; 303:893–896.4. Soutar AK, Naoumova RP. Mechanisms of disease: genetic causes of familial hypercholesterolemia. Nat Clin Pract Cardiovasc Med. 2007; 4:214–225.5. Humphries SE, Whittall RA, Hubbart CS, et al. Genetic causes of familial hypercholesterolaemia in patients in the UK: relation to plasma lipid levels and coronary heart disease risk. J Med Genet. 2006; 43:943–949.6. Marks D, Thorogood M, Neil HA, Humphries SE. A review on the diagnosis, natural history, and treatment of familial hypercholesterolaemia. Atherosclerosis. 2003; 168:1–14.7. Austin MA, Hutter CM, Zimmern RL, Humphries SE. Familial hypercholesterolemia and coronary heart disease: a HuGE association review. Am J Epidemiol. 2004; 160:421–429.8. Williams RR, Hunt SC, Schumacher MC, et al. Diagnosing heterozygous familial hypercholesterolemia using new practical criteria validated by molecular genetics. Am J Cardiol. 1993; 72:171–176.9. Yuan G, Wang J, Hegele RA. Heterozygous familial hypercholesterolemia: an underrecognized cause of early cardiovascular disease. CMAJ. 2006; 174:1124–1129.10. Scientific Steering Committee on behalf of the Simon Broome Register Group. Mortality in treated heterozygous familial hypercholesterolaemia: implications for clinical management. Atherosclerosis. 1999; 142:105–112.11. Sibley C, Stone NJ. Familial hypercholesterolemia: a challenge of diagnosis and therapy. Cleve Clin J Med. 2006; 73:57–64.12. Umans-Eckenhausen MA, Defesche JC, Sijbrands EJ, Scheerder RL, Kastelein JJ. Review of first 5 years of screening for familial hypercholesterolaemia in the Netherlands. Lancet. 2001; 357:165–168.13. Huijgen R, Vissers MN, Defesche JC, Lansberg PJ, Kastelein JJ, Hutten BA. Familial hypercholesterolemia: current treatment and advances in management. Expert Rev Cardiovasc Ther. 2008; 6:567–581.14. Cholesterol Treatment Trialists' (CTT) Collaboration. Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010; 376:1670–1681.15. Akram ON, Bernier A, Petrides F, Wong G, Lambert G. Beyond LDL cholesterol, a new role for PCSK9. Arterioscler Thromb Vasc Biol. 2010; 30:1279–1281.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Penetrating Atherosclerotic Ulcer of the Descending Thoracic Aorta in a Patient with Heterozygote Familial Hypercholesterolemia
- A Case of Familial Hypercholesterolemia with Diabetes Mellitus
- Multiple Xanthomas in a Patient with Familial Hypercholesterolemia: A Case Report
- Intertriginous Xanthoma in an Infant with Familial Hypercholesterolemia
- Individualized Treatment for Patients With Familial Hypercholesterolemia
