Primary Cardiac Angiofibroma
- Affiliations
-
- 1Cardiology Division, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. shpark0530@yuhs.ac
- 2Department of Radiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Cardiovascular Surgery, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2224821
- DOI: http://doi.org/10.4070/kcj.2013.43.9.636
Abstract
- Cardiac Angiofibroma is an uncommon intracardiac tumor. Thus far, only 4 cases of the rare intracardiac tumor have been reported. The present case-report describes an intracardiac angiofibroma in a 57-year-old healthy female. The patient was incidentally diagnosed with a left ventricle mass during echocardiography. We performed cardiac imaging, surgical excision and histological evaluation of the mass. The angiofibroma demonstrated features different from the relatively common cardiac tumors such as fibroma, myxoma and angiosarcoma. The cardiac MRI showed slightly high signal intensity on both T1 and T2, with the central core of lower signal intensity. The resected tumor was a whitish and rubbery mass. Histologically, the tumor showed the benign vascular proliferations associated with the surrounding collagen deposition.
Keyword
MeSH Terms
Figure
-

Fig. 1 A: T1 weighted image shows high signal intensity (arrow). B: T2 weighted image shows high signal intensity (arrow). C: delayed enhancement (phase-sensitive inversion recovery MR image) shows stong enhancement with central sparing (arrow). D: transthoracic echocardiographic images: four chamber view shown. It shows round shaped and echogenic mass attached at the left ventricular apex (arrow).
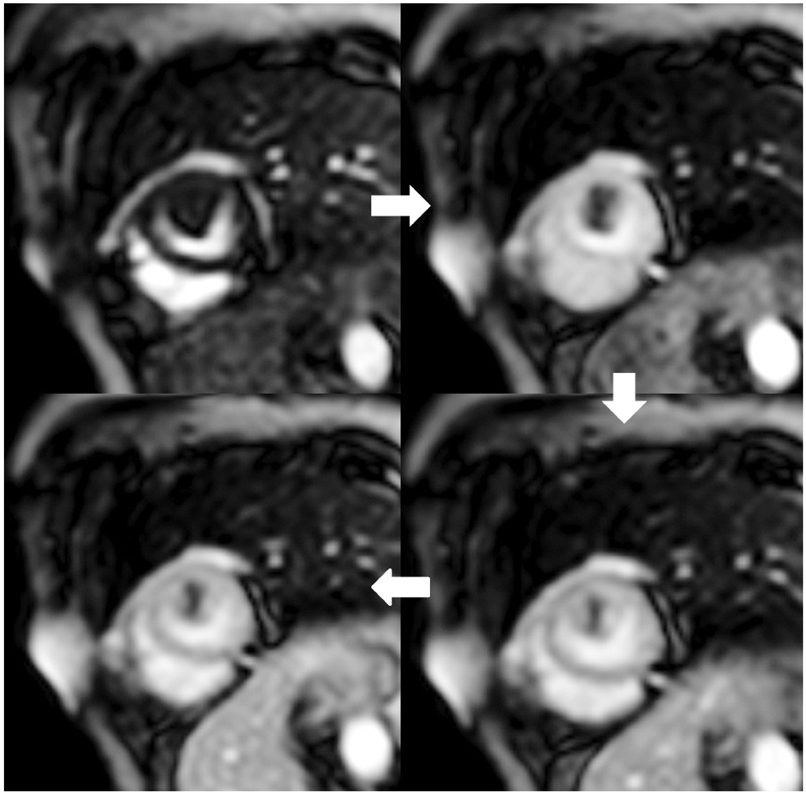
Fig. 2 Gd-DTPA first pass perfusion MRI in short axis view. The lesion shows centripetal enhancement pattern (clockwise from top left).

Fig. 3 On gross examination, a whitish, solid mass is detached from the base of the anterolateral papillary muscle.
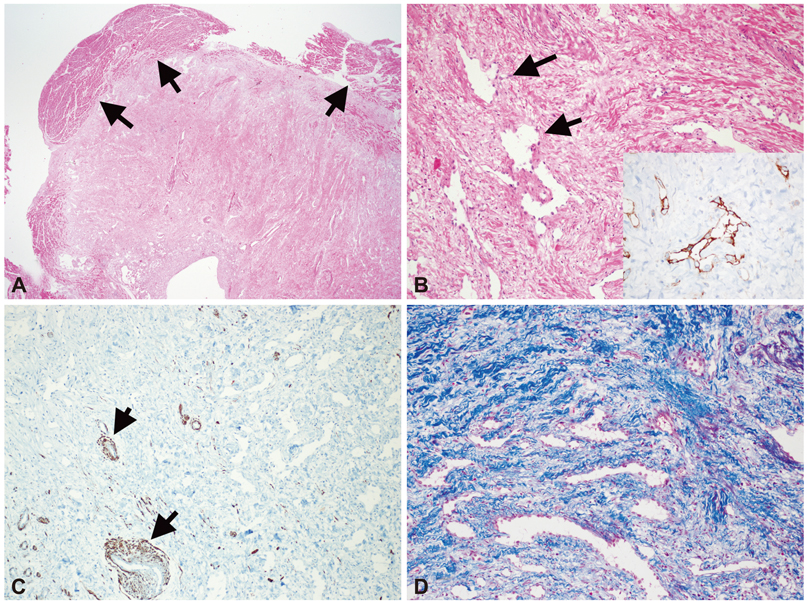
Fig. 4 A: on lower power view, the mass is somewhat well demarcated. And the mass seems to be originated from myocardium (arrows) (H-E, ×12). B: high power view shows multiple irregular vascular spaces (arrows) with intervening wavy eosinophilic collagen deposition (H-E, ×100). The vascular spaces express CD31 immunoreactivity (CD31 ×400 inlet). C: desmin immunohistochemical staining reveals that most of stroma do not express desmin except smooth muscles around vessel (arrows) (Desmin ×100). D: most of the stroma shows bluish staining on trichrome (trichrome ×100). Desmin and trichrome staining confirms that most of stroma consists of collagen, not smooth muscle.
Reference
-
1. Butany J, Nair V, Naseemuddin A, Nair GM, Catton C, Yau T. Cardiac tumours: diagnosis and management. Lancet Oncol. 2005; 6:219–228.2. Funari M, Fujita N, Peck WW, Higgins CB. Cardiac tumors: assessment with Gd-DTPA enhanced MR imaging. J Comput Assist Tomogr. 1991; 15:953–958.3. Brechtel K, Reddy GP, Higgins CB. Cardiac fibroma in an infant: magnetic resonance imaging characteristics. J Cardiovasc Magn Reson. 1999; 1:159–161.4. Jutley RS, Janas R, Matuszewski M, Suvarna K, Locke TJ. Angiofibroma of the tricuspid valve: a rare presentation of the tuberous sclerosis complex? J Cardiovasc Surg (Torino). 2006; 47:481–482.5. Satgé D, Vidalo E, Desfarges F, de Geeter B. A third case of cardiac neoplasm in a fetus with Beckwith-Wiedemann syndrome: epicardial angiofibroma. Fetal Diagn Ther. 2005; 20:44–47.6. Cao DB, Yang SR, Gao YS, Hua SC. Angiofibroma in the right atrium and inferior vena cava. Eur J Cardiothorac Surg. 2012; 41:962.7. Kirillov MM, Arkhangel'skiĭ AV, Ivanovskiĭ GI, Kuz'mina NIu. [Endocardial angiofibroma simulating a mitral heart defect]. Klin Med (Mosk). 1986; 64:120–123.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Angiofibroma Developed in the Orbit
- A Case of Extranasopharyngeal Angiofibroma Arising from the Inferior Turbinate Removed without Pre-Operative Embolization
- A Case of Extranasopharyngeal Angiofibroma of the Inferior Turbinate
- A Case of Angiofibroma Arising from the Middle Turbinate of an Adult Woman
- Congenital Fibrous Papule of the Face
