Korean Circ J.
2014 Mar;44(2):89-96. 10.4070/kcj.2014.44.2.89.
Impact of Pheochromocytoma on Left Ventricular Hypertrophy and QTc Prolongation: Comparison with Takotsubo Cardiomyopathy
- Affiliations
-
- 1Cardiovascular Research Institute, Kosin University School of Medicine, Busan, Korea. kyoungim74@gmail.com
- KMID: 2223897
- DOI: http://doi.org/10.4070/kcj.2014.44.2.89
Abstract
- BACKGROUND AND OBJECTIVES
Excessive catecholamine causes the alteration of cardiac structure and function. This study evaluated if there is any difference in left ventricular hypertrophy (LVH) and QTc prolongation in conditions with pheochromocytoma and Takotsubo cardiomyopathy (TC).
SUBJECTS AND METHODS
We reviewed the medical records of 20 pheochromocytoma patients for cardiovascular events prior to diagnosis. The patient's clinical history and electrocardiographic and echocardiographic findings were compared to those of 20 patients diagnosed with TC.
RESULTS
Left ventricular (LV) mass index (133.3+/-37.8 vs. 113.3+/-17.3, p=0.031), relative wall thickness (0.55+/-0.15 vs. 0.47+/-0.07, p=032) and elevated blood pressure (BP) were more prominent in pheochromocytoma compared to TC. The mean creatinine kinase-MB elevation, reduced LV systolic function and ST segment changes were more prominent in the TC group compared to the pheochromocytoma groups (all p<0.05). The prevalence of QTc prolongation was high in patients with pheochromocytoma (45%) and TC (55%), and TC male patients appeared to have a more prolonged QTc interval. Urine epinephrine (r=0.844, p=0.004) and norepinephrine level (r=0.782, p=0.013) were significantly correlated with LV mass index, and the predictors for the QTc prolongation were male gender and the presence of LVH.
CONCLUSION
A prolonged QTc was prominent in pheochromocytoma and TC regardless of BP and systolic LV function, and LVH was more prominent in pheochromocytoma than TC.
MeSH Terms
Figure
-
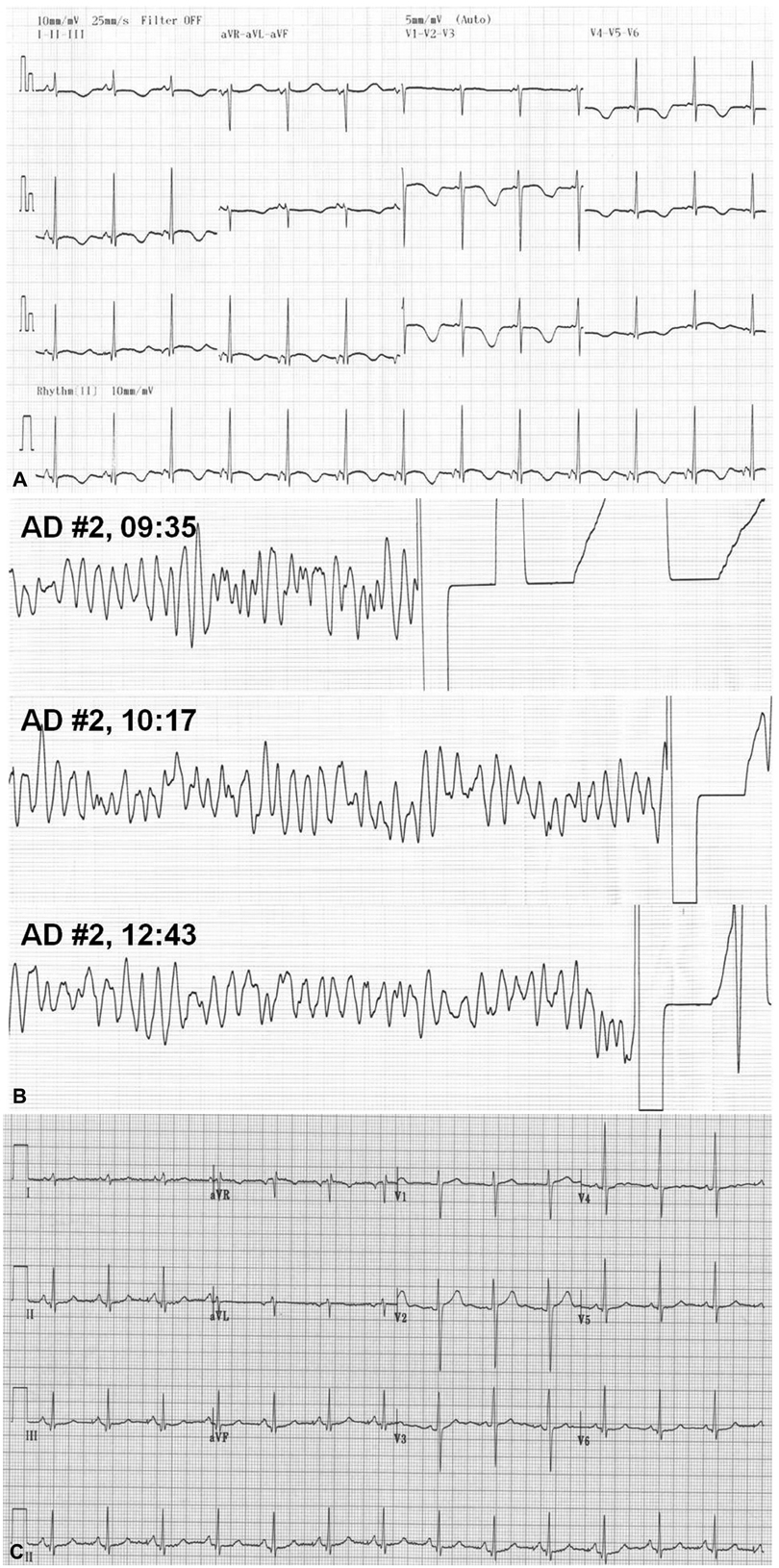
Fig. 1 Electrocardiography (ECG) of a patient with prominent QTc prolongation. The patient complained of intermittent palpitation and diaphoresis with syncope for 4 years. A: her ECG on admission showed normal sinus rhythm with a prolonged QTc interval (596 msec). B: two days after admission, a sudden onset of chest pain and syncope with loss of consciousness occurred abruptly, and ECG monitoring indicated torsades de pointes. C: after right adrenal gland removal, her electrocardiography returned to normal.
Reference
-
1. Whalen RK, Althausen AF, Daniels GH. Extra-adrenal pheochromocytoma. J Urol. 1992; 147:1–10.2. Amar L, Servais A, Gimenez-Roqueplo AP, Zinzindohoue F, Chatellier G, Plouin PF. Year of diagnosis, features at presentation, and risk of recurrence in patients with pheochromocytoma or secreting paraganglioma. J Clin Endocrinol Metab. 2005; 90:2110–2116.3. Prejbisz A, Lenders JW, Eisenhofer G, Januszewicz A. Cardiovascular manifestations of phaeochromocytoma. J Hypertens. 2011; 29:2049–2060.4. Leite LR, Macedo PG, Santos SN, Quaglia L, Mesas CE, De Paola A. Life-threatening cardiac manifestations of pheochromocytoma. Case Rep Med. 2010; 2010:976120.5. Sacha J, Wester A, Hordynski G, Pluta W. QT interval prolongation during ECG evolution in takotsubo cardiomyopathy poses a threat of torsade de pointes to predisposed patients. Case report of a female patient with congenital AV block. Herz. 2013; 38:790–795.6. van der Heide K, de Haes A, Wietasch GJ, Wiesfeld AC, Hendriks HG. Torsades de pointes during laparoscopic adrenalectomy of a pheochromocytoma: a case report. J Med Case Rep. 2011; 5:368.7. Chakraborty P, Bhattacharjeee HK, Anandaraja S. Palpitition, presyncope and abdominal mass. Indian Heart J. 2010; 62:447–448.8. Takizawa M, Kobayakawa N, Uozumi H, et al. A case of transient left ventricular ballooning with pheochromocytoma, supporting pathogenetic role of catecholamines in stress-induced cardiomyopathy or takotsubo cardiomyopathy. Int J Cardiol. 2007; 114:e15–e17.9. Agarwal V, Kant G, Hans N, Messerli FH. Takotsubo-like cardiomyopathy in pheochromocytoma. Int J Cardiol. 2011; 153:241–248.10. Matsuoka K, Okubo S, Fujii E, et al. Evaluation of the arrhythmogenecity of stress-induced "Takotsubo cardiomyopathy" from the time course of the 12-lead surface electrocardiogram. Am J Cardiol. 2003; 92:230–233.11. Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986; 57:450–458.12. Ganau A, Devereux RB, Roman MJ, et al. Patterns of left ventricular hypertrophy and geometric remodeling in essential hypertension. J Am Coll Cardiol. 1992; 19:1550–1558.13. Hannan PJ, Crow RS. Concerning the units for the QT interval corrected by Bazett's formula. Circulation. 1997; 96:3799.14. Gifford RW Jr, Bravo EL, Manger WM. Diagnosis and management of pheochromocytoma. Cardiology. 1985; 72:Suppl 1. 126–130.15. Giavarini A, Chedid A, Bobrie G, Plouin PF, Hagège A, Amar L. Acute catecholamine cardiomyopathy in patients with phaeochromocytoma or functional paraganglioma. Heart. 2013; 99:1438–1444.16. Zelinka T, Petrák O, Turková H, et al. High incidence of cardiovascular complications in pheochromocytoma. Horm Metab Res. 2012; 44:379–384.17. Eisenhofer G, Rivers G, Rosas AL, Quezado Z, Manger WM, Pacak K. Adverse drug reactions in patients with phaeochromocytoma: incidence, prevention and management. Drug Saf. 2007; 30:1031–1062.18. Bybee KA, Prasad A. Stress-related cardiomyopathy syndromes. Circulation. 2008; 118:397–409.19. Kaese S, Schülke C, Fischer D, Lebiedz P. Pheochromocytoma-induced takotsubo-like cardiomyopathy and global heart failure with need for extracorporal life support. Intensive Care Med. 2013; 39:1473–1474.20. Radtke WE, Kazmier FJ, Rutherford BD, Sheps SG. Cardiovascular complications of pheochromocytoma crisis. Am J Cardiol. 1975; 35:701–705.21. Kelm M, Schäfer S, Mingers S, et al. Left ventricular mass is linked to cardiac noradrenaline in normotensive and hypertensive patients. J Hypertens. 1996; 14:1357–1364.22. Simpson P. Norepinephrine-stimulated hypertrophy of cultured rat myocardial cells is an alpha 1 adrenergic response. J Clin Invest. 1983; 72:732–738.23. Fouad-Tarazi FM, Imamura M, Bravo EL, et al. Differences in left ventricular structural and functional changes between pheochromocytoma and essential hypertension. Role of elevated circulating catecholamines. Am J Hypertens. 1992; 5:134–140.24. Shub C, Cueto-Garcia L, Sheps SG, Ilstrup DM, Tajik AJ. Echocardiographic findings in pheochromocytoma. Am J Cardiol. 1986; 57:971–975.25. Goldbaum TS, Henochowicz S, Mustafa M, Blunda M, Lindsay J Jr. Pheochromocytoma presenting with Prinzmetal's angina. Am J Med. 1986; 81:921–922.26. Cheng TO, Bashour TT. Striking electrocardiographic changes associated with pheochromocytoma. Masquerading as ischemic heart disease. Chest. 1976; 70:397–399.27. Yu R, Nissen NN, Bannykh SI. Cardiac complications as initial manifestation of pheochromocytoma: frequency, outcome, and predictors. Endocr Pract. 2012; 18:483–492.28. Ahn JH, Park SH, Shin WY, et al. Long QT syndrome and torsade de pointes associated with Takotsubo cardiomyopathy. J Korean Med Sci. 2011; 26:959–961.29. Insulander P, Vallin H. Gender differences in electrophysiologic effects of mental stress and autonomic tone inhibition: a study in health individuals. J Cardiovasc Electrophysiol. 2005; 16:59–63.30. Panikkath R, Reinier K, Uy-Evanado A, et al. Electrocardiographic predictors of sudden cardiac death in patients with left ventricular hypertrophy. Ann Noninvasive Electrocardiol. 2013; 18:225–229.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Reversal of Takotsubo Cardiomyopathy in Patient with Pheochromocytoma
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
- A Case of Malignant Pheochromocytoma Presenting as Inverted Takotsubo-Like Cardiomyopathy
- Takotsubo Cardiomyopathy related to Pheochromocytoma or Other Etiology Should Be Considered as Similar
- A case of pheochromocytoma presenting as inverted Takotsubo cardiomyopathy
