Korean Circ J.
2014 Sep;44(5):307-311. 10.4070/kcj.2014.44.5.307.
The Presence of Fragmented QRS on 12-Lead Electrocardiography in Patients with Coronary Artery Ectasia
- Affiliations
-
- 1Turkey Yuksek Ihtisas Education and Research Hospital, Cardiology Clinic, Ankara, Turkey. sametyilmazmd@gmail.com
- KMID: 2223869
- DOI: http://doi.org/10.4070/kcj.2014.44.5.307
Abstract
- BACKGROUND AND OBJECTIVES
Coronary artery ectasia (CAE) is an angiographic finding characterized by dilation of an arterial segment with a diameter at least 1.5 times that of its adjacent normal coronary artery. Fragmented QRS (fQRS) complexes are electrocardiographic signals which reflect altered ventricular conduction around regions of a myocardial scar and/or ischaemia. In the present study, we aimed to evaluate the presence of fQRS in patients with CAE.
SUBJECTS AND METHODS
The study population included 100 patients with isolated CAE without coronary artery disease (CAD) and 80 angiographically normal controls. fQRS was defined as the presence of an additional R wave or notching of R or S wave or the presence of fragmentation in two contiguous leads corresponding to a major coronary artery territory.
RESULTS
The two groups were similar in terms of age, sex, hypertension, dyslipidemia, and family history of CAD. The presence of fQRS was significantly (p<0.05) higher in the CAE group than that in the normal coronary artery group (29% vs. 6.2%, p=0.008). Isolated CAE were detected most commonly in the right coronary artery (61%), followed by left anterior descending artery (52%), left circumflex artery (36%), and left main artery (9%). Multivariate stepwise logistic regression analysis showed that CAE {odds ratio (OR) 1.412; 95% confidence interval (CI) 1.085-1.541; p=0.003} and diabetes (OR 1.310; 95% CI 1.025-1.482; p=0.041) were independently associated with fQRS.
CONCLUSION
The presence of fragmented QRS associated with increased risk for arrhythmias and cardiovascular mortality was significantly higher in patients with CAE than in patient with normal coronary artery. Further studies are needed to determine whether the presence of fragmented QRS is a possible new risk factor for patients with CAE.
Keyword
MeSH Terms
Figure
-
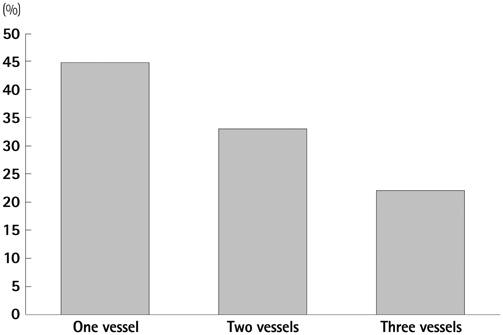
Fig. 1 Coronary artery ectasia and number of coronary vessels involved.
Reference
-
1. Satran A, Bart BA, Henry CR, et al. Increased prevalence of coronary artery aneurysms among cocaine users. Circulation. 2005; 111:2424–2429.2. Li JJ, He JG, Nan JL, He ZX, Zhu CG, Li J. Is systemic inflammation responsible for coronary artery ectasia? Int J Cardiol. 2008; 130:e69–e70.3. Falsetti HL, Carrol RJ. Coronary artery aneurysm. A review of the literature with a report of 11 new cases. Chest. 1976; 69:630–636.4. Befeler B, Aranda MJ, Embi A, Mullin FL, El-Sherif N, Lazzara R. Coronary artery aneurysms: study of the etiology, clinical course and effect on left ventricular function and prognosis. Am J Med. 1977; 62:597–607.5. Krüger D, Stierle U, Herrmann G, Simon R, Sheikhzadeh A. Exercise-induced myocardial ischemia in isolated coronary artery ectasias and aneurysms ("dilated coronopathy"). J Am Coll Cardiol. 1999; 34:1461–1470.6. Mattern AL, Baker WP, McHale JJ, Lee DE. Congenital coronary aneurysms with angina pectoris and myocardial infarction treated with saphenous vein bypass graft. Am J Cardiol. 1972; 30:906–909.7. Akyürek O, Berkalp B, Sayin T, Kumbasar D, Kervancioğlu C, Oral D. Altered coronary flow properties in diffuse coronary artery ectasia. Am Heart J. 2003; 145:66–72.8. Tigen K, Karaahmet T, Gurel E, et al. The utility of fragmented QRS complexes to predict significant intraventricular dyssynchrony in non-ischemic dilated cardiomyopathy patients with a narrow QRS interval. Can J Cardiol. 2009; 25:517–522.9. Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J. Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease. Circulation. 2006; 113:2495–2501.10. Michael MA, El Masry H, Khan BR, Das MK. Electrocardiographic signs of remote myocardial infarction. Prog Cardiovasc Dis. 2007; 50:198–208.11. Das MK, Saha C, El Masry H, et al. Fragmented QRS on a 12-lead ECG: a predictor of mortality and cardiac events in patients with coronary artery disease. Heart Rhythm. 2007; 4:1385–1392.12. Take Y, Morita H, Toh N, et al. Identification of high-risk syncope related to ventricular fibrillation in patients with Brugada syndrome. Heart Rhythm. 2012; 9:752–759.13. Das MK, Maskoun W, Shen C, et al. Fragmented QRS on twelve-lead electrocardiogram predicts arrhythmic events in patients with ischemic and nonischemic cardiomyopathy. Heart Rhythm. 2010; 7:74–80.14. Markis JE, Joffe CD, Cohn PF, Feen DJ, Herman MV, Gorlin R. Clinical significance of coronary arterial ectasia. Am J Cardiol. 1976; 37:217–222.15. Aydin M, Tekin IO, Dogan SM, et al. The levels of tumor necrosis factor-alpha and interleukin-6 in patients with isolated coronary artery ectasia. Mediators Inflamm. 2009; 2009:106145.16. Dogan A, Tuzun N, Turker Y, Akcay S, Kaya S, Ozaydin M. Matrix metalloproteinases and inflammatory markers in coronary artery ectasia: their relationship to severity of coronary artery ectasia. Coron Artery Dis. 2008; 19:559–563.17. Finkelstein A, Michowitz Y, Abashidze A, Miller H, Keren G, George J. Temporal association between circulating proteolytic, inflammatory and neurohormonal markers in patients with coronary ectasia. Atherosclerosis. 2005; 179:353–359.18. Aboeata AS, Sontineni SP, Alla VM, Esterbrooks DJ. Coronary artery ectasia: current concepts and interventions. Front Biosci (Elite Ed). 2012; 4:300–310.19. Huang QJ, Liu J, Chen MH, Li JJ. Relation of diabetes to coronary artery ectasia: a meta-analysis study. Anadolu Kardiyol Derg. 2014; 14:322–327.20. Boles U, Eriksson P, Zhao Y, Henein MY. Coronary artery ectasia: remains a clinical dilemma. Coron Artery Dis. 2010; 21:318–320.21. Farto e Abreu P, Mesquita A, Silva JA, Seabra-Gomes R. [Coronary artery ectasia: clinical and angiographic characteristics and prognosis]. Rev Port Cardiol. 1993; 12:305–310.22. Priori SG, Gasparini M, Napolitano C, et al. Risk stratification in Brugada syndrome: results of the PRELUDE (PRogrammed ELectrical stimUlation preDictive valuE) registry. J Am Coll Cardiol. 2012; 59:37–45.23. Das MK, Suradi H, Maskoun W, et al. Fragmented wide QRS on a 12-lead ECG: a sign of myocardial scar and poor prognosis. Circ Arrhythm Electrophysiol. 2008; 1:258–268.24. Femenia F, Arce M, Arrieta M, Baranchuk A. Surface fragmented QRS in a patient with hypertrophic cardiomyopathy and malignant arrhythmias: is there an association? J Cardiovasc Dis Res. 2012; 3:32–35.25. Sha J, Zhang S, Tang M, Chen K, Zhao X, Wang F. Fragmented QRS is associated with all-cause mortality and ventricular arrhythmias in patient with idiopathic dilated cardiomyopathy. Ann Noninvasive Electrocardiol. 2011; 16:270–275.26. Baranchuk A, Miranda R, Femenia F. FECHA Investigators. Chagas' cardiomyopathy and Fragmented QRS. Re: QRS fragmentation as a marker of arrhythmias in coronary artery disease, in cardiomyopathies and ion channel diseases. Int J Cardiol. 2012; 160:151–152.27. Haraoka K, Morita H, Saito Y, et al. Fragmented QRS is associated with torsades de pointes in patients with acquired long QT syndrome. Heart Rhythm. 2010; 7:1808–1814.28. Das MK, Zipes DP. Fragmented QRS: a predictor of mortality and sudden cardiac death. Heart Rhythm. 2009; 6:3 Suppl. S8–S14.29. Nagata K, Kawasaki T, Okamoto A, et al. Effectiveness of an antiplatelet agent for coronary artery ectasia associated with silent myocardial ischemia. Jpn Heart J. 2001; 42:249–254.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Independent Relationship of Systemic Inflammation With Fragmented QRS Complexes in Patients With Acute Coronary Syndromes
- Fragmented QRS and abnormal creatine kinase-MB are predictors of coronary artery disease in patients with angina and normal electrocardiographys
- QRS complex
- Various 12-Lead Electrocardiographic Findings of Diffuse Three Vessel Coronary Artery Spasm
- Absence and Resolution of Fragmented QRS Predict Reversible Myocardial Ischemia With Higher Probability of ST Segment Resolution in Patients With ST Segment Elevation Myocardial Infarction
