Intramural Reentrant Ventricular Tachycardia in a Patient with Severe Hypertensive Left Ventricular Hypertrophy
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan. epsachen@ms41.hinet.net
- 2Institute of Clinical Medicine, and Cardiovascular Research Center, National Yang-Ming University, Taipei, Taiwan.
- KMID: 2223793
- DOI: http://doi.org/10.4070/kcj.2015.45.6.526
Abstract
- We describe the case of a patient with severe hypertensive left ventricular hypertrophy and sustained hemodynamically unstable ventricular tachycardia (VT). Entrainment was demonstrated in the electrophysiological study. Activation mapping and pacemapping identified the location of the intramural reentrant VT with the exit site close to the epicardium. However, VT persisted after ablation at the epicardial exit site. Successful ablation was performed endocardially at the corresponding position.
MeSH Terms
Figure
-
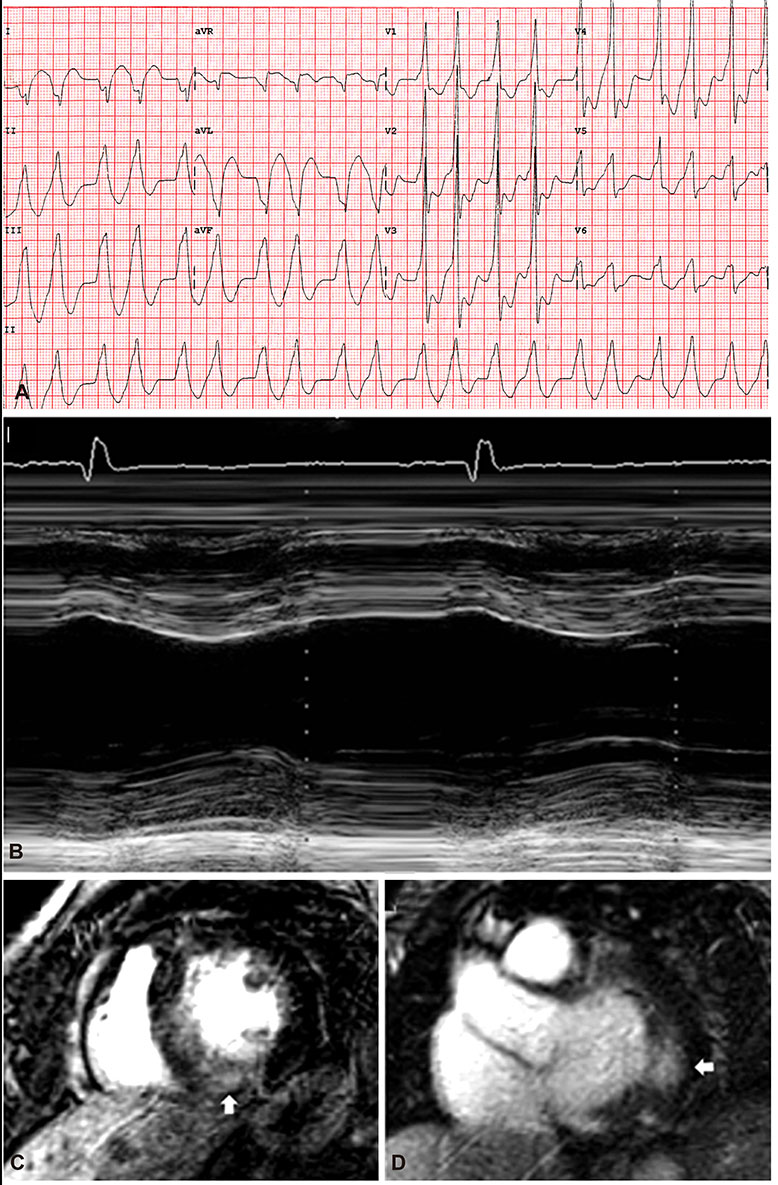
Fig. 1 Electrocardiographic morphologies of ventricular arrhythmia and echocardiography in a patient with severe concentric left ventricular hypertrophy (LVH). (A) Ventricular tachycardia (VT) ECG demonstrates a right bundle branch block, positive precordial concordance, and inferior axis with the presence of a pseudo-delta wave, high maximum deflection index, q wave in lead I, suggesting the tachycardia originating from the basal lateral mitral area epicardially. Alternation of VT cycle length with variation of QRS morphologies is noted. (B) Echocardiography reveals severe concentric LVH (intraventricular septum at diastole/posterior wall at diastole: 17/18 mm); cardiac magnetic resonance imaging shows subendocardial late gadolinium enhancement in the posterior septum, posteroinferior wall (C, arrow) and basal lateral wall (D, arrow) of the LV. LV: left ventricle, ECG: electrocardiography.

Fig. 2 The voltage mapping (upper panel) and (Pace Mapping Software, PASO; Biosense Webster, Inc., Diamond Bar, CA, USA) mapping (lower panel) demonstrated the best pacemapping site at the epicardial basal lateral mitral annulus with globally normal voltage. The local electrograms of the irrigated tip catheter (Thermocool, Biosense Webster Inc., Diamond Bar, CA, USA) at the epicardium but not at the endocardium preceded the ventricular ectopy by 33 msec.
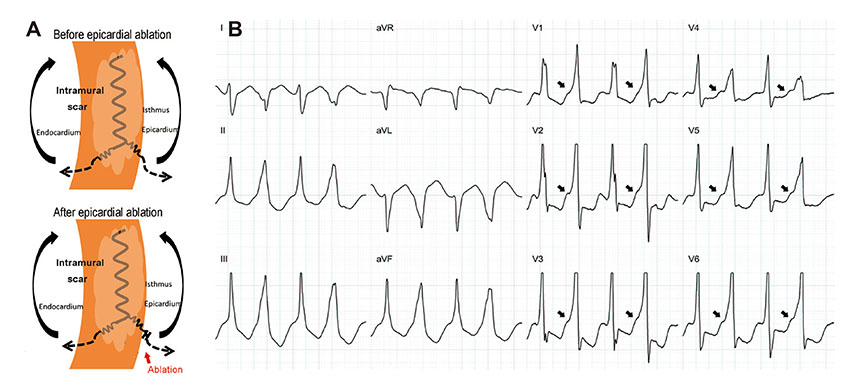
Fig. 3 Changing morphology during ventricular tachycardia. (A) Illustration demonstrates change in the ventricular tachycardia (VT) exit site from the epicardium to the endocardium and epicardial alterns after epicardial ablation. (B) Epicardial ablation results in variation of VT ECG morphology and cycle length. Presence of pseudo-delta waves (arrow) in the even beats but not in the odd bests suggest the VT exit to the epicardium and endocardium alternatively. ECG: electrocardiography.
Reference
-
1. Frohlich ED, Apstein C, Chobanian AV, et al. The heart in hypertension. N Engl J Med. 1992; 327:998–1008.2. Kannel WB, Doyle JT, McNamara PM, Quickenton P, Gordon T. Precursors of sudden coronary death. Factors related to the incidence of sudden death. Circulation. 1975; 51:606–613.3. McLenachan JM, Henderson E, Morris KI, Dargie HJ. Ventricular arrhythmias in patients with hypertensive left ventricular hypertrophy. N Engl J Med. 1987; 317:787–792.4. Dunn FG, Pringle SD. Left ventricular hypertrophy and myocardial ischemia in systemic hypertension. Am J Cardiol. 1987; 60:19I–22I.5. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990; 322:1561–1566.6. Kannel WB, Castelli WP, McNamara PM, McKee PA, Feinleib M. Role of blood pressure in the development of congestive heart failure. The Framingham study. N Engl J Med. 1972; 287:781–787.7. Galinier M, Balanescu S, Fourcade J, et al. Prognostic value of ventricular arrhythmias in systemic hypertension. J Hypertens. 1997; 15(12 Pt 2):1779–1783.8. Vallès E, Bazan V, Marchlinski FE. ECG criteria to identify epicardial ventricular tachycardia in nonischemic cardiomyopathy. Circ Arrhythm Electrophysiol. 2010; 3:63–71.9. Hutchinson MD, Gerstenfeld EP, Desjardins B, et al. Endocardial unipolar voltage mapping to detect epicardial ventricular tachycardia substrate in patients with nonischemic left ventricular cardiomyopathy. Circ Arrhythm Electrophysiol. 2011; 4:49–55.10. Lorell BH, Carabello BA. Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation. 2000; 102:470–479.11. Messerli FH, Ventura HO, Elizardi DJ, Dunn FG, Frohlich ED. Hypertension and sudden death. Increased ventricular ectopic activity in left ventricular hypertrophy. Am J Med. 1984; 77:18–22.12. Pringle SD, Dunn FG, Macfarlane PW, McKillop JH, Lorimer AR, Cobbe SM. Significance of ventricular arrhythmias in systemic hypertension with left ventricular hypertrophy. Am J Cardiol. 1992; 69:913–917.13. Ghali JK, Kadakia S, Cooper RS, Liao YL. Impact of left ventricular hypertrophy on ventricular arrhythmias in the absence of coronary artery disease. J Am Coll Cardiol. 1991; 17:1277–1282.14. Dukkipati SR, d'Avila A, Soejima K, et al. Long-term outcomes of combined epicardial and endocardial ablation of monomorphic ventricular tachycardia related to hypertrophic cardiomyopathy. Circ Arrhythm Electrophysiol. 2011; 4:185–194.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influence of left ventricular hypertrophy on ventricular arrhythmias in hypertensive patients
- Interrelated Atrioventricular Reentrant Tachycardia and Idiopathic Left Ventricular Tachycardia in a Patient with Manifested Bystander Accessory Pathway
- A Comparative Study of Left Ventricular Diastolic Function between Hypertrophic Cardiomyopathy and Hypertensive Patients with Left Ventricular Hypertrophy
- Effect of Left Ventricular Hypertrophy on Ventricular Performance in Essential Hypertension
- Left Ventricular Diastolic Functions by M-Mode Echocardiogram in Essential Hypertensive Patients
