Diffuse Skeletal Hemangiomatosis Mimicking Sacroiliitis
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. sybang@hanyang.ac.kr
- 2Department of Radiology, Hanyang University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Hanyang University College of Medicine, Seoul, Korea.
- 4Department of Orthopedic Surgery, Hanyang University College of Medicine, Seoul, Korea.
- KMID: 2222963
- DOI: http://doi.org/10.4078/jrd.2014.21.4.205
Abstract
- Hemangiomatosis of the skeletal system is a rare disease without specific symptoms and signs. We describe a 20-year-old patient with low back pain, whose plain radiographs of sacroiliac (SI) joint showed irregular sclerotic lesions. The patient was finally confirmed with skeletal hemangiomatosis by magnetic resonance imaging (MRI) and excisional biopsy of the lesion. The present case suggests that if patients with abnormal lesions of the SI joint in the plain radiographs do not have typical inflammatory back pain, advanced imaging is required to make an accurate diagnosis. Our case also emphasizes the importance of MRI and biopsy in establishing the diagnosis.
MeSH Terms
Figure
-

Figure 1. (A) X-ray showing irregular sclerotic lesions of the left SI joint (arrowheads), and sclerotic cystic lesions in the both sacral wing and left ilium (arrows). (B) Sclerotic changes of vertebral endplates in a lumbar spine X-ray. (C) Pelvic bone CT scan showing sclerotic cystic lesions in the sacral wing and left ilium (arrows). (D) MRI of the SI joints showing subchondral, cortical, intramedul-lary osseous cysts (arrows). (E) In the T1 weighted and T2 weighted MRI images of the L-spine, multiple T1 low, T2 high signal intensities are scattered from the T9 to the S3 vertebra. (F) In fat suppression images the lesions appear as high signal intensities, and are markedly enhanced after gadolinium administration. (G) CT scan showing multiple irregularly-shaped fat-containing lesions in the thoracolumbar vertebrae, sacrum, and left iliac bone (arrows) and multiple cystic mass lesions in the spleen (arrowheads).
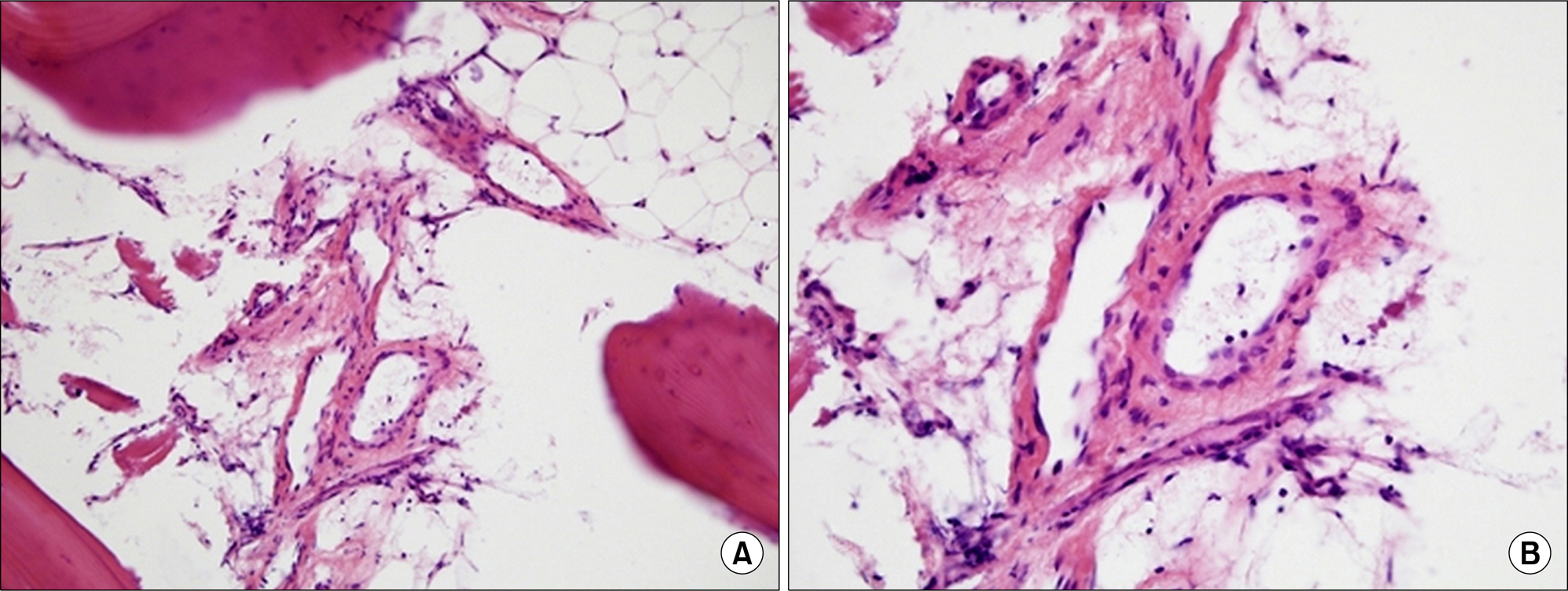
Figure 2. Histologic appearance of a bone lesion (hematoxylin-eosin ×200 (A) and ×400 (B)) shows bony trabecula with some medium-sized abnormal vessels in fatty marrow spaces.
Reference
-
1. Dorfman HD, Steiner GC, Jaffe HL. Vascular tumors of bone. Hum Pathol. 1971; 2:349–76.
Article2. Chawla A, Singrakhia M, Maheshwari M, Modi N, Parmar H. Intraosseous haemangioma of the proximal femur: imaging findings. Br J Radiol. 2006; 79:e64–6.
Article3. Heckl S, Aschoff A, Kunze S. Cavernomas of the skull: review of the literature 1975-2000. Neurosurg Rev. 2002; 25:56–62. discussion 66-7.
Article4. Cheng NC, Lai DM, Hsie MH, Liao SL, Chen YB. Intraosseous hemangiomas of the facial bone. Plast Reconstr Surg. 2006; 117:2366–72.
Article5. Braun J, Sieper J, Bollow M. Imaging of sacroiliitis. Clin Rheumatol. 2000; 19:51–7.6. Koito K, Namieno T, Nagakawa T, Morita K. Balloon-oc-cluded retrograde transvenous obliteration for gastric vari-ces with gastrorenal or gastrocaval collaterals. AJR Am J Roentgenol. 1996; 167:1317–20.
Article7. Ogose A, Hotta T, Morita T, Takizawa T, Ohsawa H, Hirata Y. Solitary osseous hemangioma outside the spinal and craniofacial bones. Arch Orthop Trauma Surg. 2000; 120:262–6.
Article8. Puig J, Garcia-Pena P, Enriquez G, Huguet P, Lucaya J. Intraosseous haemangioma of the ilium. Pediatr Radiol. 2006; 36:54–6.
Article9. Kaleem Z, Kyriakos M, Totty WG. Solitary skeletal hemangioma of the extremities. Skeletal Radiol. 2000; 29:502–13.
Article10. Laredo JD, Assouline E, Gelbert F, Wybier M, Merland JJ, Tubiana JM. Vertebral hemangiomas: fat content as a sign of aggressiveness. Radiology. 1990; 177:467–72.
Article11. Yamamoto T, Kurosaka M, Mizuno K. Juxtaarticular hemangioma of long bone. Skeletal Radiol. 2000; 29:535–7.
Article12. Hermann KG, Braun J, Fischer T, Reisshauer H, Bollow M. Magnetic resonance tomography of sacroiliitis: anatomy, histological pathology, MR-morphology, and grading. Radiologe. 2004; 44:217–28.13. Rudwaleit M, Khan MA, Sieper J. The challenge of diagnosis and classification in early ankylosing spondylitis: do we need new criteria? Arthritis Rheum. 2005; 52:1000–8.
Article14. Jacobson JA, Girish G, Jiang Y, Sabb BJ. Radiographic evaluation of arthritis: degenerative joint disease and variations. Radiology. 2008; 248:737–47.
Article15. Canella C, Schau B, Ribeiro E, Sbaffi B, Marchiori E. MRI in seronegative spondyloarthritis: imaging features and differential diagnosis in the spine and sacroiliac joints. AJR Am J Roentgenol. 2013; 200:149–57.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diffuse Hemangiomatosis in the Intra-Abdominal Cavity Mimicking Peritoneal Metastasis: A Case Report
- Diffuse Neonatal Hemangiomatosis
- A Case of Diffuse Neonatal Hemangiomatosis Successfully Treated with Propranolol
- Diffuse Neonatal Hemangiomatosis with Association of Massive Osteolysis and Arteriovenous Fistulae: An autopsy case
- Diffuse Neonatal Hemangiomatosis with Association of Massive Osteolysis and Arteriovenous Fistulae: An autopsy case
