The Efficacy of Nailfold Capillaroscopy in Patients with Raynaud's Phenomenon
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea. healthyra@schmc.ac.kr
- KMID: 2222908
- DOI: http://doi.org/10.4078/jrd.2015.22.2.69
Abstract
- Raynaud's phenomenon (RP) is characterized by reversible digital vasospasm triggered by exposure to cold or emotional stress. It manifests with unique 'triphasic' (pallor, cyanosis, erythema) or 'biphasic' (white, blue) color change. Clinically, RP is classified as primary RP, which does not have an underlying associated cause with a relatively benign course, and secondary RP, which predates various cause such as systemic connective tissue disease (CTD). Therefore, RP must be differentiated for detection of emerging CTD such as systemic sclerosis (SSc), systemic lupus erythematosus, and mixed conective tissue disease, ect. Nailfold capillaroscopy (NFC) is a non-invasive morphological study used routinely with antinuclear antibodies for parallel of secondary RP. A recent study showed NFC to be the best predictor of transition from a primary RP to secondary RP. The well-established role of NFC for early diagnosis of SSc, and potential for monitoring disease progression and predictive clinical complication makes NFC an important tool in research and clinical practice. In this paper, I present a recent update with emphasis on its possible role as a reliable diagnostic tool and biomarker in secondary RP.
MeSH Terms
Figure
-

Figure 1. Three-step approach to diagnosis of primary Raynaud's phenomenon (RP). If 3 or more criteria met from step 3, then the patient has RP. Cited from the article of Maverakis et al. (J Autoimmun 2014;48-49:60-5) [12].
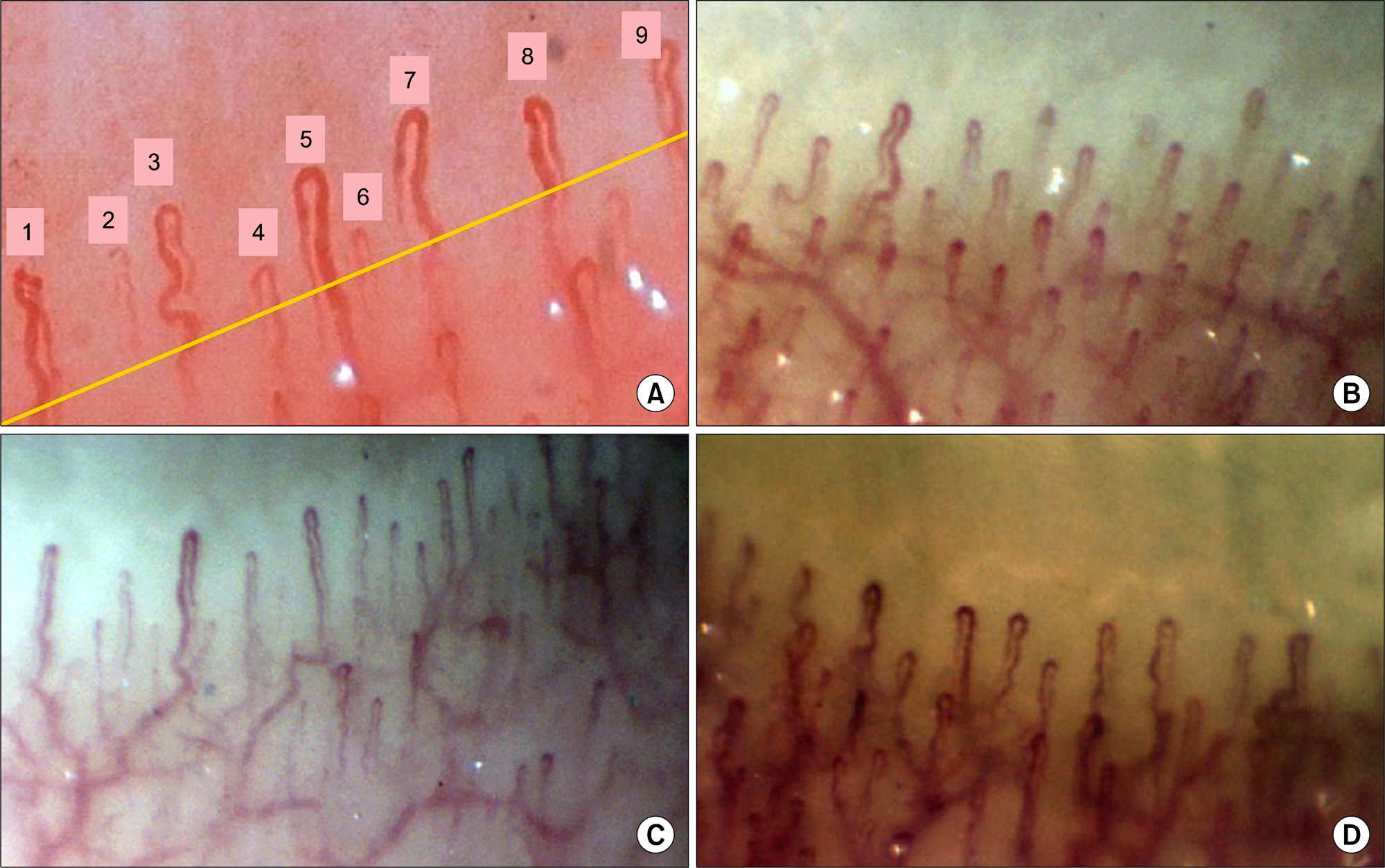
Figure 2. The examples of nailfold capillaroscopic finding in healthy subjects (×200) [15,28]. (A) For counting the total number of capillaries in 1 mm, we should check the number of the loop that exceeded a half line of mean capillary length. The capillary number is 9/mm. (B, C) It shows ‘perfect normal patterns' with >5 U-shaped loops/mm. Increasing subvenous capillary plexus can be visible in normal persons. (D) It shows ‘within normal pattern' mainly compatible criteria with 2∼5 U-shaped loops/mm and ≤2 tortuous loops/mm.

Figure 3. The example of nailfold capillaroscopic finding in systemic sclerosis (SSc) (×200) [9,15]. (A, B) It shows that almost capillaries are dilated and large number of megacapillaries in the early phase of SSc. (C) Typically many giant capillaries and micro-hemorrages are noted in the active phase of SSc. (D) At the late phase of SSc, avascular areas are observed along with bushy capillaries.
Cited by 1 articles
-
Case of Raynaud Syndrome after the Use of Methimazole
Yunkyung Kim, Hee-Sang Tag, Geun-Tae Kim, Seung-Geun Lee, Eun-Kyung Park, Ji-Heh Park, Seong-min Kweon, Song-I Yang, Jeong-Hoon Kim
J Rheum Dis. 2018;25(3):203-206. doi: 10.4078/jrd.2018.25.3.203.
Reference
-
1. Hong YS. Systemic sclerosis. In: Korean Colleage Rheumatology. Text book of rheumatology. 1st ed.Seoul: Koonja;2014. p. 409–11.2. Suter LG, Murabito JM, Felson DT, Fraenkel L. The incidence and natural history of Raynaud's phenomenon in the community. Arthritis Rheum. 2005; 52:1259–63.
Article3. Herrick AL. The pathogenesis, diagnosis and treatment of Raynaud phenomenon. Nat Rev Rheumatol. 2012; 8:469–79.
Article4. Cutolo M, Pizzorni C, Secchi ME, Sulli A. Capillaroscopy. Best Pract Res Clin Rheumatol. 2008; 22:1093–108.
Article5. Koenig M, Joyal F, Fritzler MJ, Roussin A, Abrahamowicz M, Boire G, et al. Autoantibodies and microvascular damage are independent predictive factors for the progression of Raynaud's phenomenon to systemic sclerosis: a twen-ty-year prospective study of 586 patients, with validation of proposed criteria for early systemic sclerosis. Arthritis Rheum. 2008; 58:3902–12.
Article6. Lombard WP. The blood pressure in the arterioles, capillaries and small veins of the human skin. Am J Physiol. 1912; 29:335–62.
Article7. Brown GE, O'Leary PA. Skin capillaries in scleroderma. Arch Intern Med (Chic). 1925; 36:73–88.
Article8. Cutolo M, Smith V. State of the art on nailfold capillaroscopy: a reliable diagnostic tool and putative biomarker in rheumatology? Rheumatology (Oxford). 2013; 52:1933–40.
Article9. Kim HS. Updated classification criteria for systemic sclerosis: the concept of early diagnosis. Korean J Med. 2014; 87:395–400.
Article10. van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013; 65:2737–47.
Article11. LeRoy EC, Medsger TA Jr. Raynaud's phenomenon: a proposal for classification. Clin Exp Rheumatol. 1992; 10:485–8.12. Maverakis E, Patel F, Kronenberg DG, Chung L, Fiorentino D, Allanore Y, et al. International consensus criteria for the diagnosis of Raynaud's phenomenon. J Autoimmun. 2014; 48-49:60–5.
Article13. Ingegnoli F, Gualtierotti R, Lubatti C, Bertolazzi C, Gutierrez M, Boracchi P, et al. Nailfold capillary patterns in healthy subjects: a real issue in capillaroscopy. Microvasc Res. 2013; 90:90–5.
Article14. Cutolo M, Sulli A, Smith V. How to perform and interpret capillaroscopy. Best Pract Res Clin Rheumatol. 2013; 27:237–48.
Article15. Allen J. Capillaroscopy in healthy subjects of different ages. Cutolo M, Smith V, Sulli A, editors. Atlas of capillaroscopy in rheumatic diseases. Milano: Elsevier Srl cop;2010. p. 49–54.16. Spencer-Green G. Outcomes in primary Raynaud phenomenon: a meta-analysis of the frequency, rates, and predictors of transition to secondary diseases. Arch Intern Med. 1998; 158:595–600.17. Ingegnoli F, Boracchi P, Gualtierotti R, Lubatti C, Meani L, Zahalkova L, et al. Prognostic model based on nailfold capillaroscopy for identifying Raynaud's phenomenon patients at high risk for the development of a scleroderma spectrum disorder: PRINCE (prognostic index for nailfold capillaroscopic examination). Arthritis Rheum. 2008; 58:2174–82.
Article18. Ingegnoli F, Boracchi P, Gualtierotti R, Biganzoli EM, Zeni S, Lubatti C, et al. Improving outcome prediction of systemic sclerosis from isolated Raynaud's phenomenon: role of autoantibodies and nailfold capillaroscopy. Rheumatology (Oxford). 2010; 49:797–805.
Article19. Pavlov-Dolijanovic SR, Damjanov NS, Vujasinovic Stupar NZ, Baltic S, Babic DD. The value of pattern capillary changes and antibodies to predict the development of systemic sclerosis in patients with primary Raynaud's phenomenon. Rheumatol Int. 2013; 33:2967–73.
Article20. Schneeberger D, Tyndall A, Kay J, Søndergaard KH, Carreira PE, Morgiel E, et al. Systemic sclerosis without antinuclear antibodies or Raynaud's phenomenon: a multicentre study in the prospective EULAR Scleroderma Trials and Research (EUSTAR) database. Rheumatology (Oxford). 2013; 52:560–7.
Article21. Matucci-Cerinic M, Kahaleh B, Wigley FM. Review: evidence that systemic sclerosis is a vascular disease. Arthritis Rheum. 2013; 65:1953–62.
Article22. Subcommittee for scleroderma criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee. Preliminary criteria for the classification of systemic sclerosis (scleroderma). Arthritis Rheum. 1980; 23:581–90.23. Singh JA, Solomon DH, Dougados M, Felson D, Hawker G, Katz P, et al. Classification and Response Criteria Subcommittee of the Committee on Quality Measures, American College of Rheumatology. Development of classification and response criteria for rheumatic diseases. Arthritis Rheum. 2006; 55:348–52.24. LeRoy EC, Medsger TA Jr. Criteria for the classification of early systemic sclerosis. J Rheumatol. 2001; 28:1573–6.25. Maricq HR, LeRoy EC, D'Angelo WA, Medsger TA Jr, Rodnan GP, Sharp GC, et al. Diagnostic potential of in vivo capillary microscopy in scleroderma and related disorders. Arthritis Rheum. 1980; 23:183–9.
Article26. Cutolo M, Sulli A, Smith V. Assessing microvascular changes in systemic sclerosis diagnosis and management. Nat Rev Rheumatol. 2010; 6:578–87.
Article27. Valentini G, Marcoccia A, Cuomo G, Vettori S, Iudici M, Bondanini F, et al. Early systemic sclerosis: analysis of the disease course in patients with marker autoantibody and/or capillaroscopic positivity. Arthritis Care Res (Hoboken). 2014; 66:1520–7.
Article28. Kim HS, Park MK, Kim HY, Park SH. Capillary dimension measured by computer-based digitalized image correlated with plasma endothelin-1 levels in patients with systemic sclerosis. Clin Rheumatol. 2010; 29:247–54.
Article29. Kallenberg CG, Wouda AA, Hoet MH, van Venrooij WJ. Development of connective tissue disease in patients presenting with Raynaud's phenomenon: a six year follow up with emphasis on the predictive value of antinuclear anti-bodies as detected by immunoblotting. Ann Rheum Dis. 1988; 47:634–41.
Article30. Ingegnoli F, Ardoino I, Boracchi P, Cutolo M. EUSTAR co-authors. Nailfold capillaroscopy in systemic sclerosis: data from the EULAR scleroderma trials and research (EUSTAR) database. Microvasc Res. 2013; 89:122–8.
Article31. Caramaschi P, Canestrini S, Martinelli N, Volpe A, Pieropan S, Ferrari M, et al. Scleroderma patients nailfold video-capillaroscopic patterns are associated with disease subset and disease severity. Rheumatology (Oxford). 2007; 46:1566–9.
Article32. Sebastiani M, Manfredi A, Vukatana G, Moscatelli S, Riato L, Bocci M, et al. Predictive role of capillaroscopic skin ulcer risk index in systemic sclerosis: a multicentre validation study. Ann Rheum Dis. 2012; 71:67–70.
Article33. Hofstee HM, Vonk Noordegraaf A, Voskuyl AE, Dijkmans BA, Postmus PE, Smulders YM, et al. Nailfold capillary density is associated with the presence and severity of pulmonary arterial hypertension in systemic sclerosis. Ann Rheum Dis. 2009; 68:191–5.
Article34. Greidinger EL, Gaine SP, Wise RA, Boling C, Housten-Harris T, Wigley FM. Primary pulmonary hypertension is not associated with scleroderma-like changes in nailfold capillaries. Chest. 2001; 120:796–800.
Article35. Ohtsuka T, Hasegawa A, Nakano A, Yamakage A, Yamaguchi M, Miyachi Y. Nailfold capillary abnormality and pulmonary hypertension in systemic sclerosis. Int J Dermatol. 1997; 36:116–22.
Article36. Kayser C, Sekiyama JY, Próspero LC, Camargo CZ, Andrade LE. Nailfold capillaroscopy abnormalities as predictors of mortality in patients with systemic sclerosis. Clin Exp Rheumatol. 2013; 31(2 Suppl 76):103–8.37. Ingegnoli F, Gualtierotti R. A systematic overview on the use and relevance of capillaroscopy in systemic sclerosis. Expert Rev Clin Immunol. 2013; 9:1091–7.
Article38. Choi JJ, Min DJ, Cho ML, Min SY, Kim SJ, Lee SS, et al. Elevated vascular endothelial growth factor in systemic sclerosis. J Rheumatol. 2003; 30:1529–33.39. Distler O, Del Rosso A, Giacomelli R, Cipriani P, Conforti ML, Guiducci S, et al. Angiogenic and angiostatic factors in systemic sclerosis: increased levels of vascular endothelial growth factor are a feature of the earliest disease stages and are associated with the absence of fingertip ulcers. Arthritis Res. 2002; 4:R11.40. Sulli A, Soldano S, Pizzorni C, Montagna P, Secchi ME, Villaggio B, et al. Raynaud's phenomenon and plasma endothelin: correlations with capillaroscopic patterns in systemic sclerosis. J Rheumatol. 2009; 36:1235–9.
Article41. Avouac J, Vallucci M, Smith V, Senet P, Ruiz B, Sulli A, et al. Correlations between angiogenic factors and capillaroscopic patterns in systemic sclerosis. Arthritis Res Ther. 2013; 15:R55.
Article42. Volpe A, Biasi D, Caramaschi P, Mantovani W, Bambara LM, Canestrini S, et al. Levels of F2-isoprostanes in systemic sclerosis: correlation with clinical features. Rheumatology (Oxford). 2006; 45:314–20.
Article43. Riccieri V, Stefanantoni K, Vasile M, Macrì V, Sciarra I, Iannace N, et al. Abnormal plasma levels of different angiogenic molecules are associated with different clinical manifestations in patients with systemic sclerosis. Clin Exp Rheumatol. 2011; 29(2 Suppl 65):S46–52.44. Berks M, Tresadern P, Dinsdale G, Murray A, Moore T, Herrick A, et al. An automated system for detecting and measuring nailfold capillaries. Med Image Comput Comput Assist Interv. 2014; 17:658–65.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Increased plasma endothelin-1 and abnormal nailfold capillaroscopic findings in patients with connective tissue diseases
- The Clinical Efficacy of Nailfold Capillaroscopy in Rheumatic Diseases
- Comparison between Power Doppler Ultrasonography and Nailfold Capillaroscopy for the Differentiation of Raynaud's Phenomenon
- The Clinical Significance Of Nailfold Capillary Microscopic Examination In The Patients With Co Ech Tissue Diseases
- A Diagnostic Roadmap for Raynaud's Phenomenon
