J Rheum Dis.
2015 Oct;22(5):308-312. 10.4078/jrd.2015.22.5.308.
A Case of Eosinophilic Polymyositis Treated with Immunosuppressants
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. shinseok@chonnam.ac.kr
- KMID: 2222844
- DOI: http://doi.org/10.4078/jrd.2015.22.5.308
Abstract
- Eosinophilic polymyositis is a rare form of inflammatory muscle disease associated with peripheral blood and/or tissue eosinophilia. Most patients respond to glucocorticoids, however some show poor prognosis, leading to mortality. A 28-year-old female was admitted to our hospital because of myalgia and motor weakness of the upper and lower extremities. Laboratory findings showed significantly elevated levels of muscle enzymes and inflammatory lesions in both thigh muscles were demonstrated on magnetic resonance imaging. A diagnosis of eosinophilic polymyositis was based on histological findings, which showed diffuse eosinophilic infiltration into perivascular spaces in the endomysium and perimysium, and necrosis of myofibers. High-dose methylprednisolone treatment improved the clinical symptoms and muscle enzymes. However, on tapering the glucocorticoid dose, clinical and laboratory findings were exacerbated. After the addition of methotrexate and azathioprine, the symptoms and muscle enzymes recovered without relapse. Here, we report on a case of eosinophilic polymyositis, which responded to immunosuppressants.
Keyword
MeSH Terms
-
Adult
Azathioprine
Diagnosis
Eosinophilia
Eosinophils*
Female
Glucocorticoids
Humans
Immunosuppressive Agents*
Lower Extremity
Magnetic Resonance Imaging
Methotrexate
Methylprednisolone
Mortality
Muscles
Myalgia
Myositis
Necrosis
Polymyositis*
Prognosis
Recurrence
Thigh
Azathioprine
Glucocorticoids
Immunosuppressive Agents
Methotrexate
Methylprednisolone
Figure
-
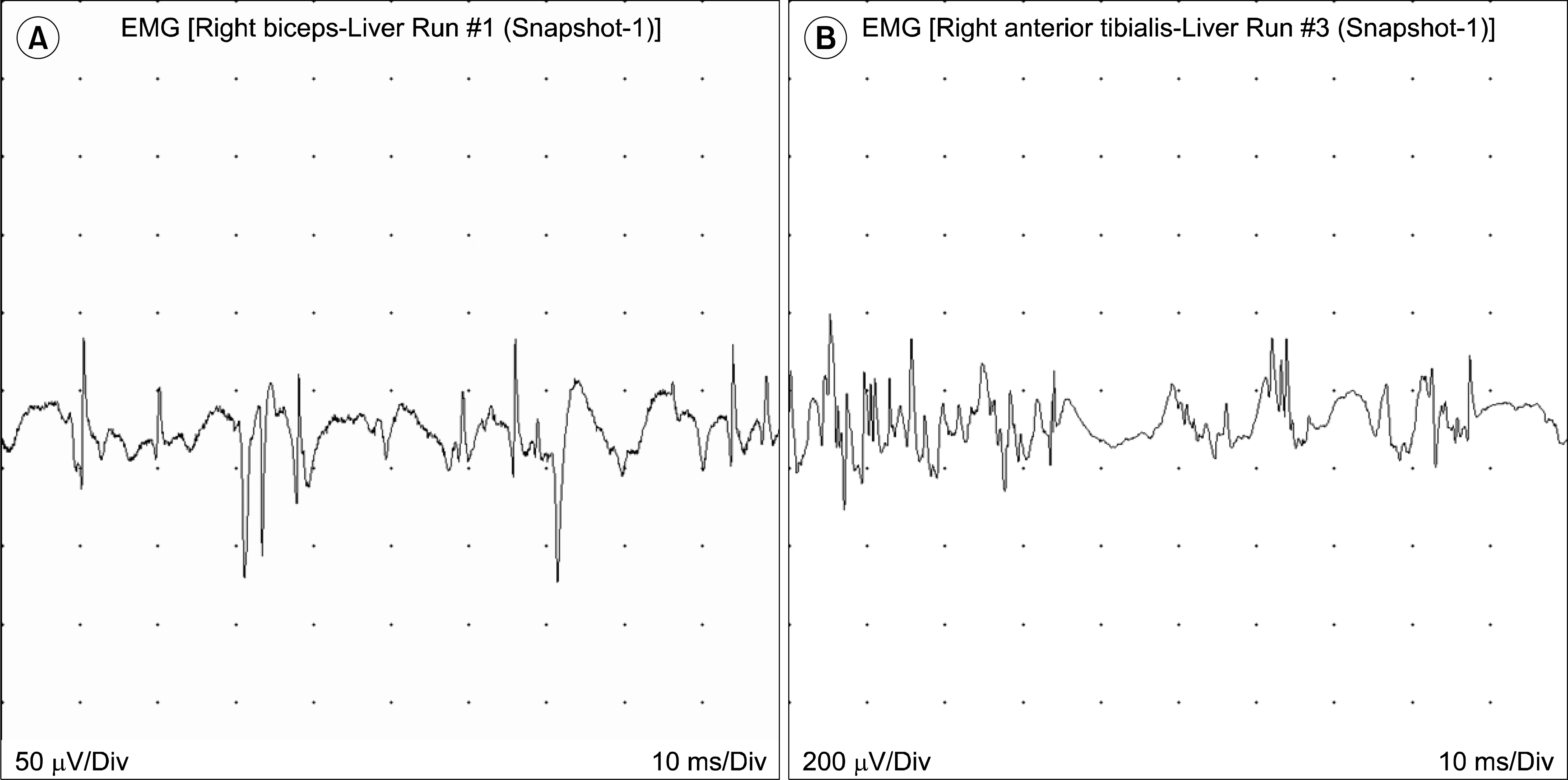
Figure 1. Electromyography (EMG) of right bicpes muscle (A) and right anterior tibialis muscle (B) show short duration and small polyphasic motor unit action potentials.
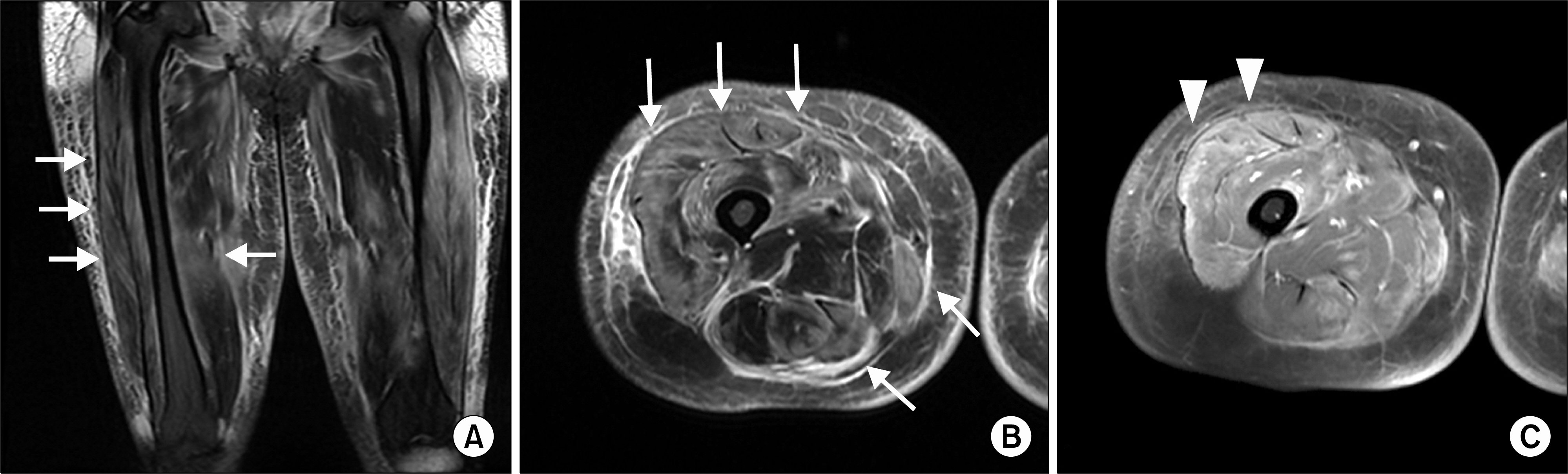
Figure 2. (A, B) T2 weighted magnetic resonance imaging of right thigh shows heterogeneous hypersignal intensity of thigh muscles and subcutaneous edema (arrows). (C) Fat suppression gadolinium enhanced axial T1 weight imaging shows heterogeneous enhancement of right thigh muscles (arrowheads).
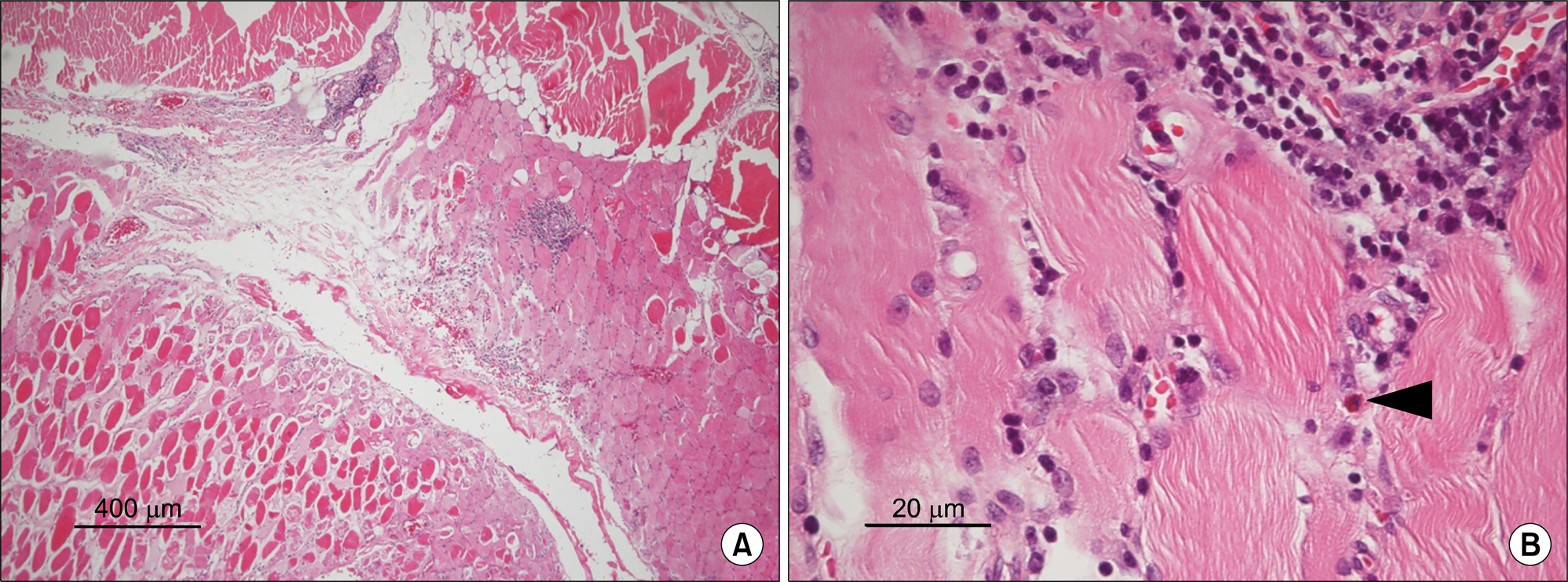
Figure 3. A hematoxylin and eosin-stained paraffin section from the right thigh muscle biopsy specimen reveals infiltration of eosinophils (arrowhead) and inflammatory cells on perivascular spaces in the endomysium and perimysium and necrosis of myofibers (A: ×40, B: ×400).
Reference
-
1. Kaufman LD, Kephart GM, Seidman RJ, Buhner D, Qvar-fordt I, Nässberger L, et al. The spectrum of eosinophilic myositis. Clinical and immunopathogenic studies of three patients, and review of the literature. Arthritis Rheum. 1993; 36:1014–24.2. Pickering MC, Walport MJ. Eosinophilic myopathic syndromes. Curr Opin Rheumatol. 1998; 10:504–10.
Article3. Hall FC, Krausz T, Walport MJ. Idiopathic eosinophilic myositis. QJM. 1995; 88:581–6.4. Amato AA. Adults with eosinophilic myositis and calpain-3 mutations. Neurology. 2008; 70:730–1.
Article5. Krahn M, Lopez de Munain A, Streichenberger N, Bernard R, Pécheux C, Testard H, et al. CAPN3 mutations in patients with idiopathic eosinophilic myositis. Ann Neurol. 2006; 59:905–11.6. Yonker RA, Panush RS. Idiopathic eosinophilic myositis with preexisting fibromyalgia. J Rheumatol. 1985; 12:165–7.7. Agrawal BL, Giesen PC. Eosinophilic myositis. An unusual cause of pseudotumor and eosinophilia. JAMA. 1981; 246:70–1.
Article8. Serratrice G, Pellissier JF, Cros D, Gastaut JL, Brindisi G. Relapsing eosinophilic perimyositis. J Rheumatol. 1980; 7:199–205.9. Sladek GD, Vasey FB, Sieger B, Behnke DA, Germain BF, Espinoza LR. Relapsing eosinophilic myositis. J Rheumatol. 1983; 10:467–70.10. Selva-O'Callaghan A, Trallero-Araguás E, Grau JM. Eosinophilic myositis: an updated review. Autoimmun Rev. 2014; 13:375–8.11. Murata K, Sugie K, Takamure M, Fujimoto T, Ueno S. Eosinophilic major basic protein and interleukin-5 in eosinophilic myositis. Eur J Neurol. 2003; 10:35–8.
Article12. Cantarini L, Volpi N, Carbotti P, Greco G, Aglianò M, Bellisai F, et al. Eosinophilia-associated muscle disorders: an immunohistological study with tissue localisation of major basic protein in distinct clinicopathological forms. J Clin Pathol. 2009; 62:442–7.
Article13. Trüeb RM, Becker-Wegerich P, Hafner J, Wüthrich B, Burg G. Relapsing eosinophilic perimyositis. Br J Dermatol. 1995; 133:109–14.14. Strosberg JM, Lava NS. Polymyositis with eosinophilia and mononeuropathy multiplex. J Rheumatol. 1981; 8:523–6.15. Stark RJ. Eosinophilc polymyositis. Arch Neurol. 1979; 36:721–2.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Eosinophilic Polymyositis in a Patient with IgA Nephropathy
- A Case of Rhabdomyolysis in Eosinophilic Polymyositis
- Eosinophilic Polymyositis and DRESS (Drug Rash with Eosinophilia and Systemic Symptoms) Syndrome by Antitubercular Agents
- Three Cases of Polymyositis Developed Associated with Chronic Liver Disease
- A Case of Hypercapnic Respiratory Failurein a Patient with Eosinophilic Polymyositis
