A Case of Nasolacrimal Duct Obstruction after Two-Jaw Surgery
- Affiliations
-
- 1Department of Ophthalmology, Chonbuk National University Medical School, Jeonju, Korea. ahnmin@jbnu.ac.kr
- KMID: 2217048
- DOI: http://doi.org/10.3341/jkos.2013.54.5.794
Abstract
- PURPOSE
To describe a case of nasolacrimal duct obstruction after two-jaw surgery.
CASE SUMMARY
A 22-year-old woman presented with a 1-year history of epiphora after two-jaw surgery. Orbital CT showed 5 mm of focal soft tissue at the level of the distal nasolacrimal duct. Dacryocystography showed complete obstruction at the nasolacrimal duct level. Thus a nasolacrimal duct obstruction was diagnosed by physical and radiologic examination.
CONCLUSIONS
In patients with epiphora who have undergone two-jaw surgery, precise examination and treatment is required in order to exclude nasolacrimal duct obstruction.
Figure
-

Figure 3. A Dacryocystography of the patient shows complete obstruction of the right nasolacrimal duct.

Figure 4. The osteotomy line of conventional Lefort surgery is shown by the dotted line. The inferior orifice of the nasolacri-mal canal (black arrow) is located at the top of the curved in-sertion of the inferior turbinate.

Figure 1. A general sequence of two-jaw surgery. After osteotomy of the maxilla and mandibule, trimming of the bone for adjustments should be done (B). Repo- sitioning of the bones (C). Bone plates and screws used for fixation of the bones (D).
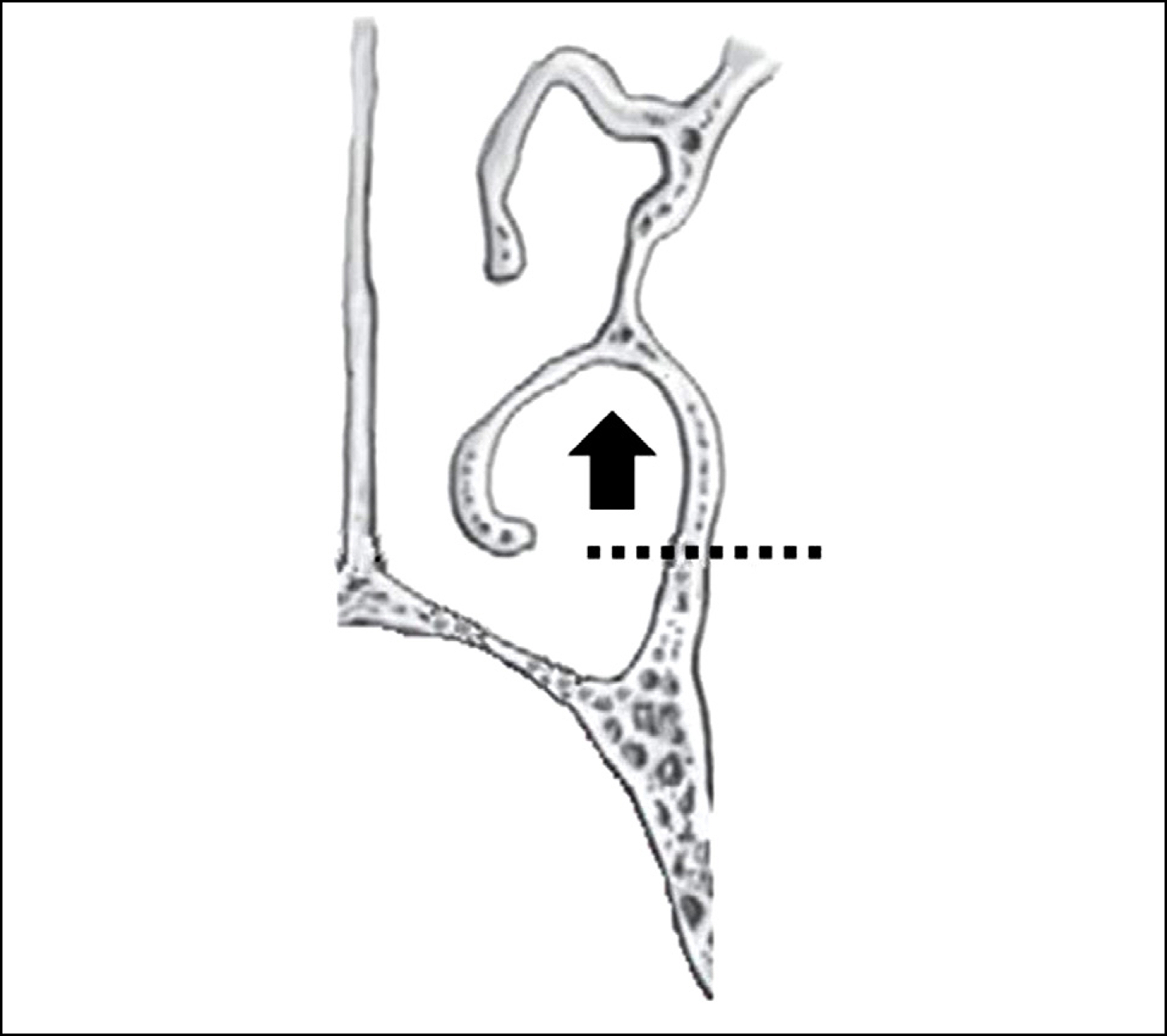
Figure 2. A continuous coro-nal section of facial CT (A-D) shows nasolacrimal duct (long arrow) and fracture line of Lefort surgery (small arrow). A right nasolacrimal duct opening is obstructed with soft tissue (D).
Reference
-
References
1. Menendez LF, Biedlingmaier JF, Tilghman D. Osteomeatal com-plex obstruction and sinusitis following Le Fort I osteotomy. J Oral Maxillofac Surg. 1996; 54:103–4.
Article2. Bruno C, Fernanda N, Belini M. Bloody tears after miniplate osteo-synthesis for Le Fort I osteotomy. Asian J Oral Maxillofac Surg. 2011; 10:1016–8.3. Shoshani Y, Samet N, Ardekian L, Taicher S. Nasolacrimal duct in-jury after Le Fort I osteotomy. J Oral Maxillofac Surg. 1994; 52:406–7.
Article4. Keller EE, Sather AH. Quadriangular Le Fort I osteotomy : Surgical technique and review of 54 patients. J Oral Maxillofac Surg. 1990; 48:2–11.5. Little C, Mintz S, Elinger AC. The distal lacrimal ductal system and traumatic epiphora. Int J Oral Maxillofac Surg. 1991; 20:31–5.
Article6. Demas PN, Sotereanos GC. Incidence of nasolacrimal injury and turbinectomy associated atrophic rhinitis with Le Fort I osteotomies. J Craniomaxillofac Surg. 1989; 17:116–8.7. You ZH, Bell WH, Finn RA. Location of the nasolacrimal canal in relation to the high Le Fort I Osteotomy. J Oral Maxillofac Surg. 1992; 50:1075–80.
Article8. Bays RA, Bouloux GF. Complications of orthognathic surgery. Oral Maxillofacial Surg Clin N Am. 2003; 15:229–42.
Article9. Kim SG, Park SS. Incidence of complications and problems related to orthognathic surgery. J Oral Maxillofac Surg. 2007; 65:2438–44.
Article10. Li KK, Meara JG, Rubin PA. Orbital compartment syndrome fol-lowing orthognathic surgery. J Oral Maxillofac Surg. 1995; 53:964–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nasolacrimal Duct Obstruction Following Midfacial Autologous Fat Injection
- A Case of Angioleiomyoma in Nasolacrimal Duct
- A Case of Nasolacrimal Duct Obstruction Caused by a Lacrimal Sac Retention Cyst
- The Methods of Insertiong the Root-type Lacrimal Tube and an Artificial nasolacrimal duct into the Men's
- Silicone Intubation for Nasolacrimal Duct Obstruction in Adult
