A Case of Superior Orbital Fissure Syndrome Induced by Penetrating Orbital Injury
- Affiliations
-
- 1Department of Ophthalmology, Chonbuk National University Medical School, Jeonju, Korea. ahnmin@jbnu.ac.kr
- 2Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 2215711
- DOI: http://doi.org/10.3341/jkos.2015.56.4.592
Abstract
- PURPOSE
We report a case of superior orbital fissure syndrome induced by penetrating orbital injury caused by a steel wire and analyzed the clinical outcomes.
CASE SUMMARY
A 49-year-old female visited our clinic after a penetrating orbital injury through the right inferolateral conjunctiva caused by a steel wire. The best corrected visual acuity of the right eye was 0.8 and a fixed dilated pupil was detected. Partial ptosis and ophthalmoplegia were observed in the right eye. The computed tomography image revealed no sign of orbital wall fracture, retrobulbar hemorrhage or foreign body. Slightly increased signal intensity was observed on the magnetic resonance image but other abnormal findings of the extraocular muscle and optic nerve were not detected. Under the impression of superior orbital fissure syndrome, systemic steroid was administered orally. After 1 month, ptosis and ophthalmoplegia were partially improved. After 3 months, the pupil size and response were normalized.
CONCLUSIONS
The oral steroid treatment was given to reduce the edema without orbital wall fracture after the penetrating orbital injury, which caused the superior orbital fissure syndrome. The symptom was relieved 3 months after the injury.
MeSH Terms
Figure
-
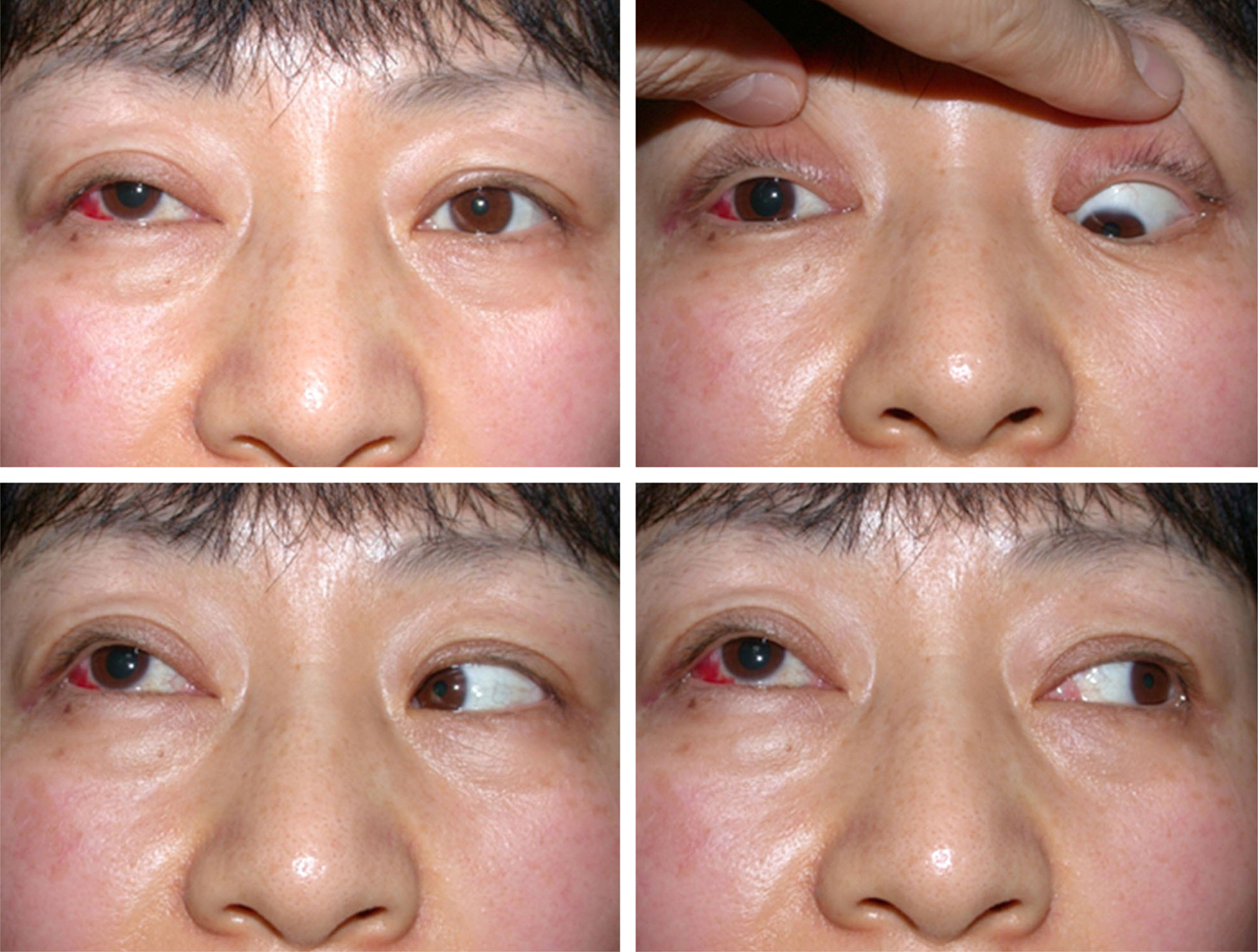
Figure 1. Ophthalmoplegia of the right eye and partial ptosis of the right upper eyelid are noted at 1 hour after the injury.

Figure 2. Injury site on the inferolateral side of right bulbar conjunctiva (arrow).
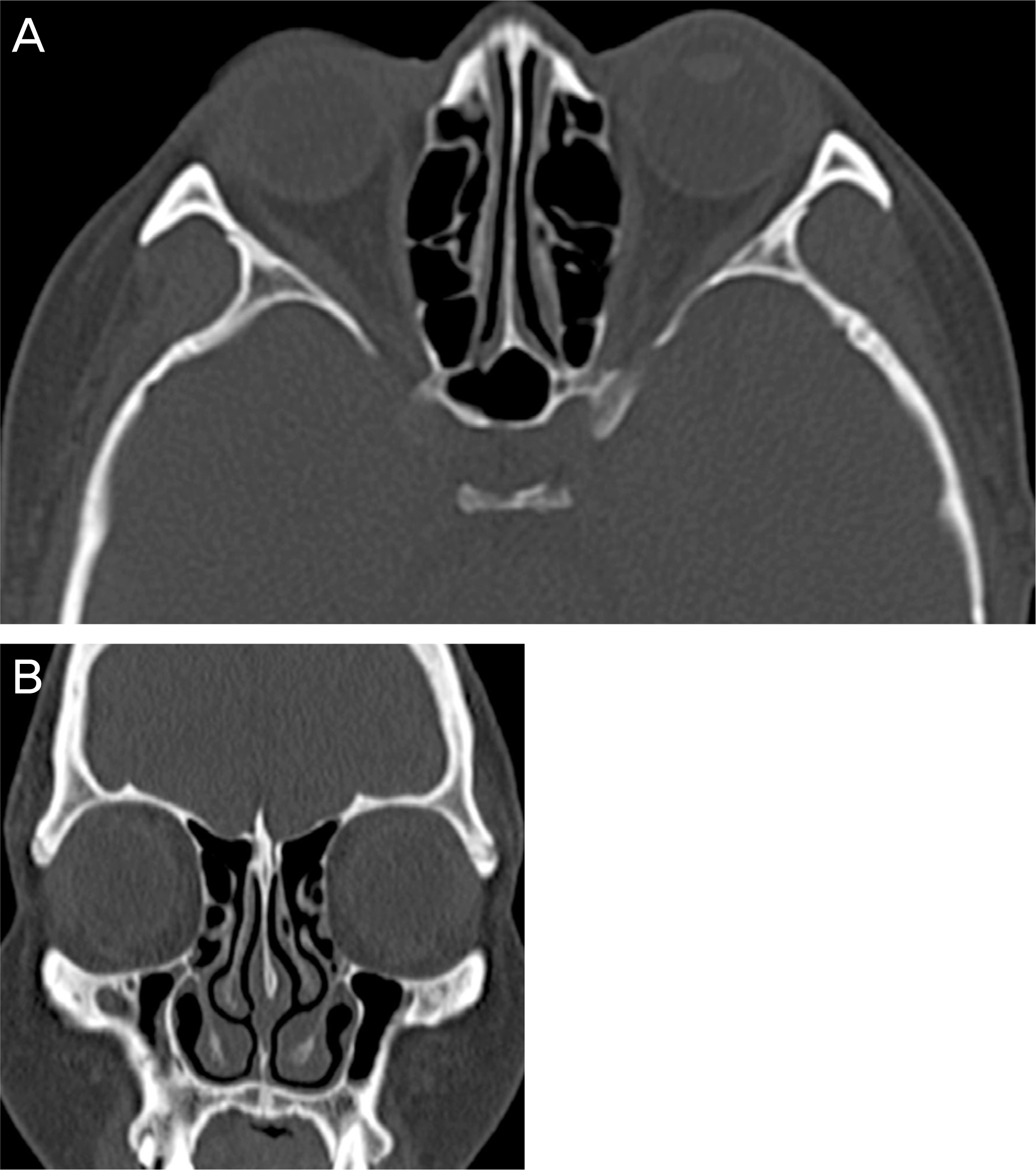
Figure 3. Axial (A) and coronal (B) CT scan at 1 hour after injury. There is no sign of orbital wall fracture, retrobulbar hemorrhage or foreign body.

Figure 4. Axial MRI (T2 weighted image) scan at 1 hour after injury. Retrobulbar soft tissue of the right eye shows slightly increased signal intensity (arrow).
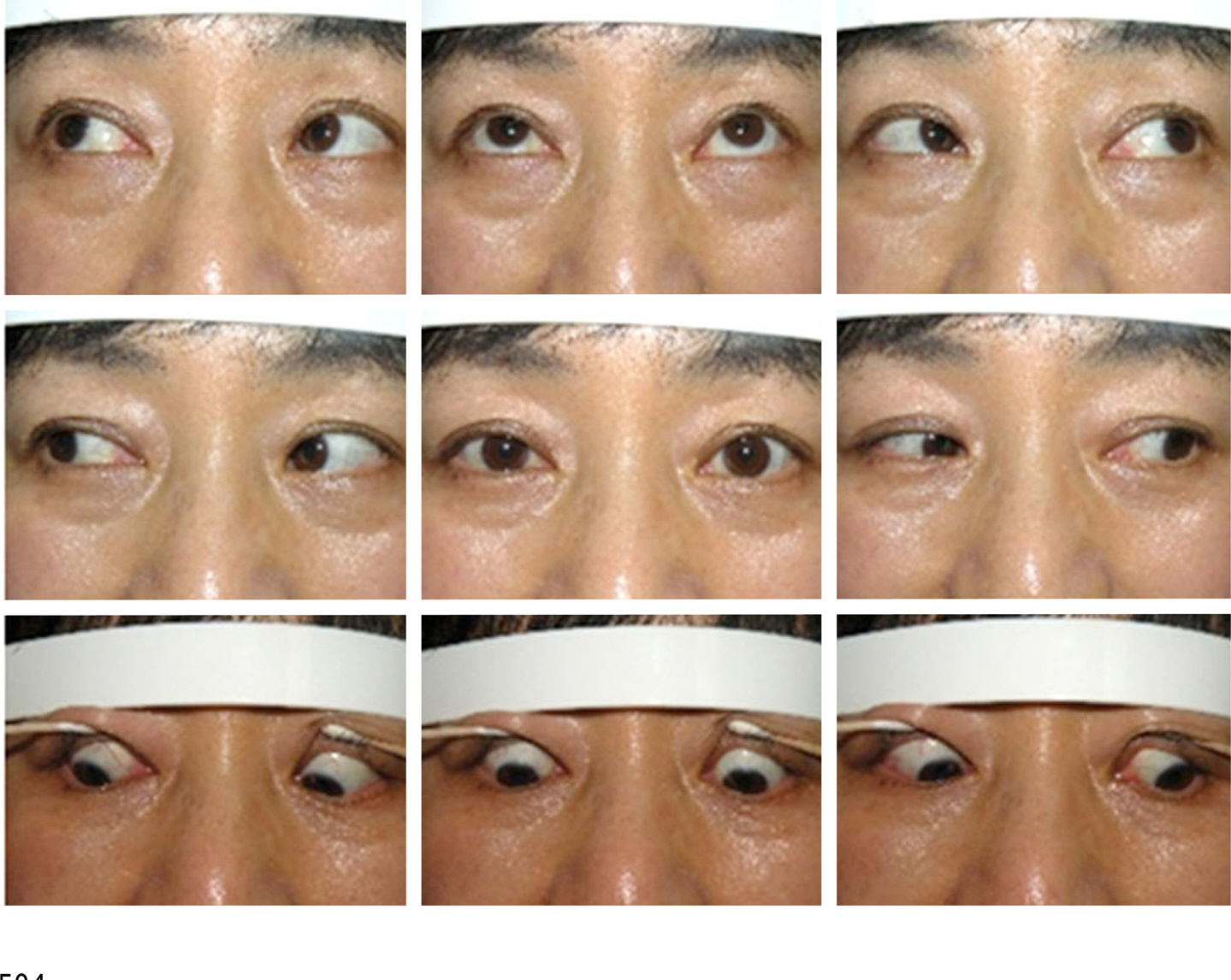
Figure 5. Fields of gazes at three months after the injury show recovery of the extraocular muscle movement in all directions. Ptosis of the right upper eyelid improved.
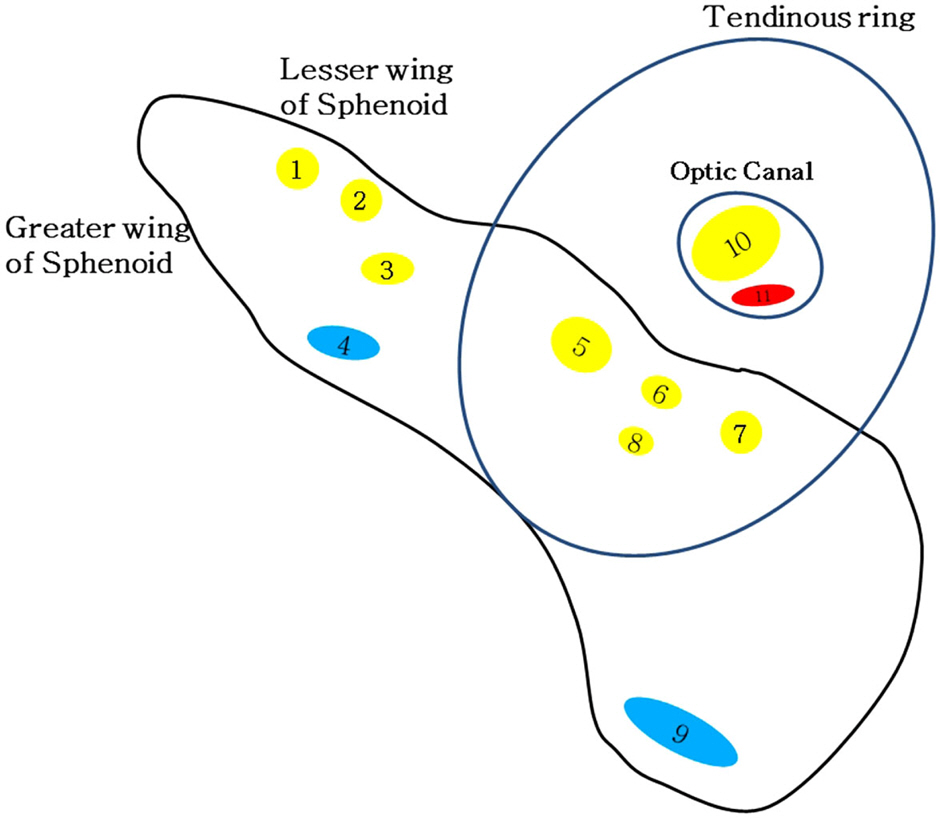
Figure 6. Diagrammatic representation of right superior orbital fissure with its contents (1. lacrimal nerve; 2. frontal nerve; 3. trochlear nerve; 4. superior branch of ophthalmic vein; 5. superior branch of oculomotor nerve; 6. nasociliary nerve; 7. inferior branch of oculomotor nerve; 8. abducens nerve; 9. inferior branch of ophthalmic vein; 10. optic nerve; 11. ophthalmic artery).
Reference
-
References
1. Chen CT, Chen YR. Traumatic superior orbital fissure syndrome: current management. Craniomaxillofac Trauma Reconstr. 2010; 3:9–16.
Article2. Hirschfeld L. Epanchement de sang dans le sinus caverneux du cote gauche diagnostique pendant la vie. Compt Rend Soc Biol. 1858; 138.3. Rai S, Rattan V. Traumatic superior orbital fissure syndrome: Review of literature and report of three cases. Natl J Maxillofac Surg. 2012; 3:222–5.
Article4. Zachariades N. The superior orbital fissure syndrome. Review of the literature and report of a case. Oral Surg Oral Med Oral Pathol. 1982; 53:237–40.5. Chen CT, Wang TY, Tsay PK, et al. Traumatic superior orbital fissure syndrome: assessment of cranial nerve recovery in 33 cases. Plast Reconstr Surg. 2010; 126:205–12.
Article6. Zachariades N, Vairaktaris E, Papavassiliou D, et al. The superior orbital fissure syndrome. J Maxillofac Surg. 1985; 13:125–8.
Article7. Antonyshyn O, Gruss JS, Kassel EE. Blow-in fractures of the orbit. Plast Reconstr Surg. 1989; 84:10–20.
Article8. Sieverink NP, van der Wal KG. Superior orbital fissure syndrome in a 7-year-old boy. Int J Oral Surg. 1980; 9:216–20.
Article9. Robinson DC, Jarrett WJ. Superior orbital fissure syndrome with Bell's palsy: report of case. J Oral Surg. 1973; 31:203–6.10. Unger JM, Gentry LR, Grossman JE. Sphenoid fractures: prevalence, sites, and significance. Radiology. 1990; 175:175–80.
Article11. Pogrel MA. The superior orbital fissure syndrome: report of case. J Oral Surg. 1980; 38:215–7.12. Bun RJ, Vissink A, Bos RR. Traumatic superior orbital fissure syndrome: report of two cases. J Oral Maxillofac Surg. 1996; 54:758–61.
Article13. Postma MP, Seldomridge GW, Vines FS. Superior orbital fissure syndrome and bilateral internal carotid pseudoaneurysms. J Oral Maxillofac Surg. 1990; 48:503–8.
Article14. Rohrich RJ, Hackney FL, Parikh RS. Superior orbital fissure syndrome: current management concepts. J Craniomaxillofac Trauma. 1995; 1:44–8.15. Levin LA, Beck RW, Joseph MP, et al. The treatment of traumatic optic neuropathy: the International Optic Nerve Trauma Study. Ophthalmology. 1999; 106:1268–77.16. Yip CC, Chng NW, Au Eong KG, et al. Low-dose intravenous methylprednisolone or conservative treatment in the management of traumatic optic neuropathy. Eur J Ophthalmol. 2002; 12:309–14.
Article17. Bracken MB, Shepard MJ, Holford TR, et al. Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA. 1997; 277:1597–604.
Article18. Chung JW, Kim SJ, Lee SY, Lee EH. A case of superior orbital fissure syndrome. J Korean Ophthalmol Soc. 2001; 42:654–7.19. Kim SG. Traumatic Superior orbital fissure syndrome complicating fractures of the facial skeleton: Report of a Case. J Korean Assoc Maxillofac Plast Reconstr Surg. 2000; 22:356–9.20. Kim YI, Paik UB, Kim JH, et al. Case report of traumatic orbital apex syndrome and superior orbital fissure syndrome. J Korean Assoc Maxillofac Plast Reconstr Surg. 1994; 15:275–80.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Superior orbital fissure syndrome complicating fractures of the facial skeleton: Report of a Case
- A case of metastatic hepatocellular carcinoma to orbit with superior orbital fissure syndrome
- Superior Orbital Fissure Syndrome after Repair of Blow Out Fracture
- A Statistical Analysis of Superior Orbital Fissure Width in Korean Adults using Computed Tomography Scans
- Traumatic Superior Orbital Fissure Syndrome: Case Report
