The Measurement of Flow Resistance in Drainage Implants Using Various Tube Ligation Methods
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea. kihopark@snu.ac.kr
- KMID: 2214582
- DOI: http://doi.org/10.3341/jkos.2011.52.5.610
Abstract
- PURPOSE
To evaluate the flow resistance though the tube in a glaucoma drainage implant using various tube ligation methods.
METHODS
To measure the flow resistance, the following tube ligation methods were designed and tested: Type 1: no ligation of Ahmed valve tube. Type 2: ligation of Ahmed valve tube with 8-0 Vicryl. Type 3: ligation of Molteno tube and a 6-0 Vicryl as an intra-luminal stent with 8-0 Vicryl. Type 4: ligation of Ahmed valve tube and three strands of 8-0 nylon as extra-luminal stents with 8-0 Vicryl. Type 5: ligation of Ahmed valve tube and a 6-0 Prolene as an extra-luminal stent with 8-0 Vicryl followed by removal of the Prolene for partial ligation.
RESULTS
The pressure was maintained under 0.143 mm Hg in type 1. In type 2, the pressure increased to 6.688 mm Hg and dropped to approximately 6.384 mm Hg. In type 3, the pressure was maintained at 5.396 mm Hg which decreased to 3.572 mm Hg after stent removal. In type 4, the pressure was maintained at 5.700 mm Hg which dropped to 5.472 mm Hg after the 1st stent removal, to 5.016 mm Hg after the 2nd stent removal and to 4.180 mm Hg after the 3rd stent removal. In type 5, the pressure increased to 6.384 mm Hg and decreased to 5.624 mm Hg.
CONCLUSIONS
The tube ligation along with extra-luminal stents followed by staged removal may provide prevention of hypotony and staged control of intraocular pressure after a glaucoma implant operation.
Keyword
MeSH Terms
Figure
-

Figure 1. Closed manometric apparatus used in this experiment for the calibration of manometer. Pig eye is connected in series with anterior chamber (A/C) cannulator, infusion pump and manometer. (A) Pig eye is given pressured on by A/C cannulator. BSS solution is flowed into pig eye with infusion pump. (B) A/C cannulator intentionally makes intraocular pressure (IOP) of pig eye the level that we want. Intraocular pressure is internally measured by manometer and external measured by rebound tonopen. Intraocular pressures measured by manometer and rebound Tono-Pen and A/C cannulator-made pressure are compared each other. (C) Infusion pump used in this experiment. (D) Manometer used in this experiment. (E) Anterior chamber (A/C) cannulator used in this experiment. (F) Rebound Tono-Pen used in this experiment.
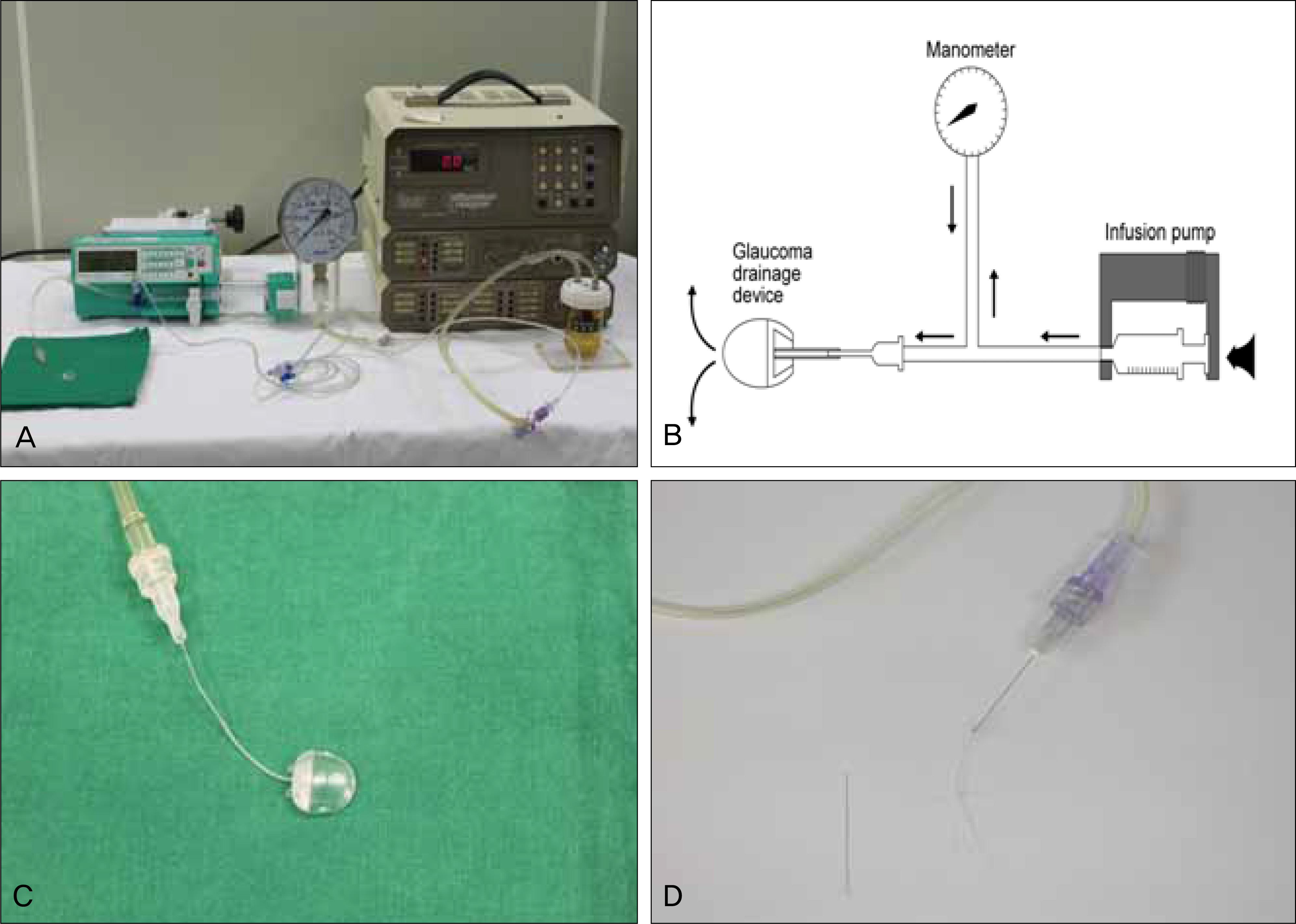
Figure 2. (A) Closed manometric apparatus to measure intraluminal pressure in the tube of glaucoma drainage devices (GDD). (B) Schematic diagram of this apparatus used in this experiment. Tube is connected in series with infusion pump and manometer. (C) Ahmed valve implant is connected with a Healon needle. (D) It is observed that a Molteno tube is connected with a Healon needle. A 6-0 Vicryl stent is found in the left side of the tube.
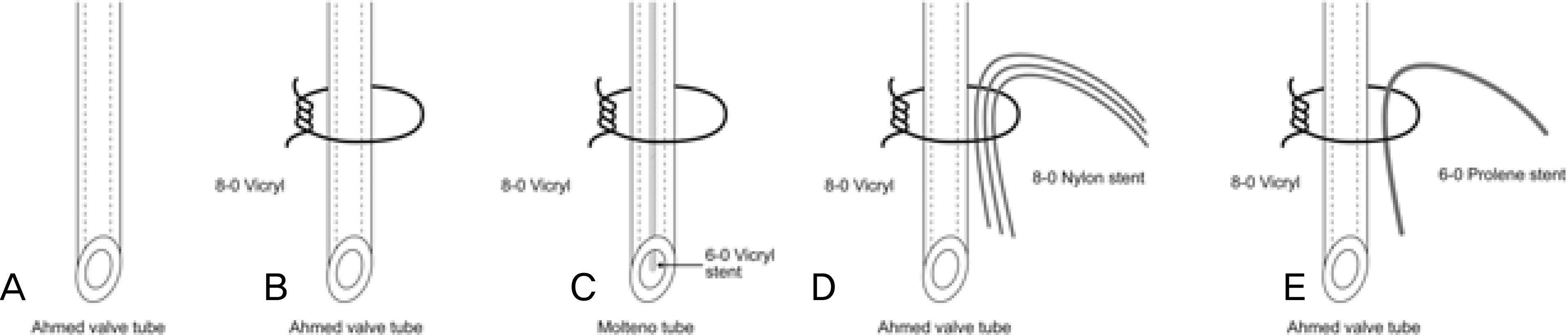
Figure 3. Various tube ligation and stent methods. (A) Type 1, no ligation of Ahmed valve tube. (B) Type 2, ligation of Ahmed valve tube with 8-0 Vicryl. (C) Type 3, ligation of Molteno tube and a 6-0 Vicryl as an intra-luminal stent with 8-0 Vicryl. (D) Type 4, ligation of Ahmed valve tube and three strands of 8-0 nylon as extra-luminal stents with 8-0 Vicryl. (E) Type 5, ligation of Ahmed valve tube and a 6-0 Prolene as an extra-luminal stent with 8-0 Vicryl and then Prolene is removed for partial ligation.
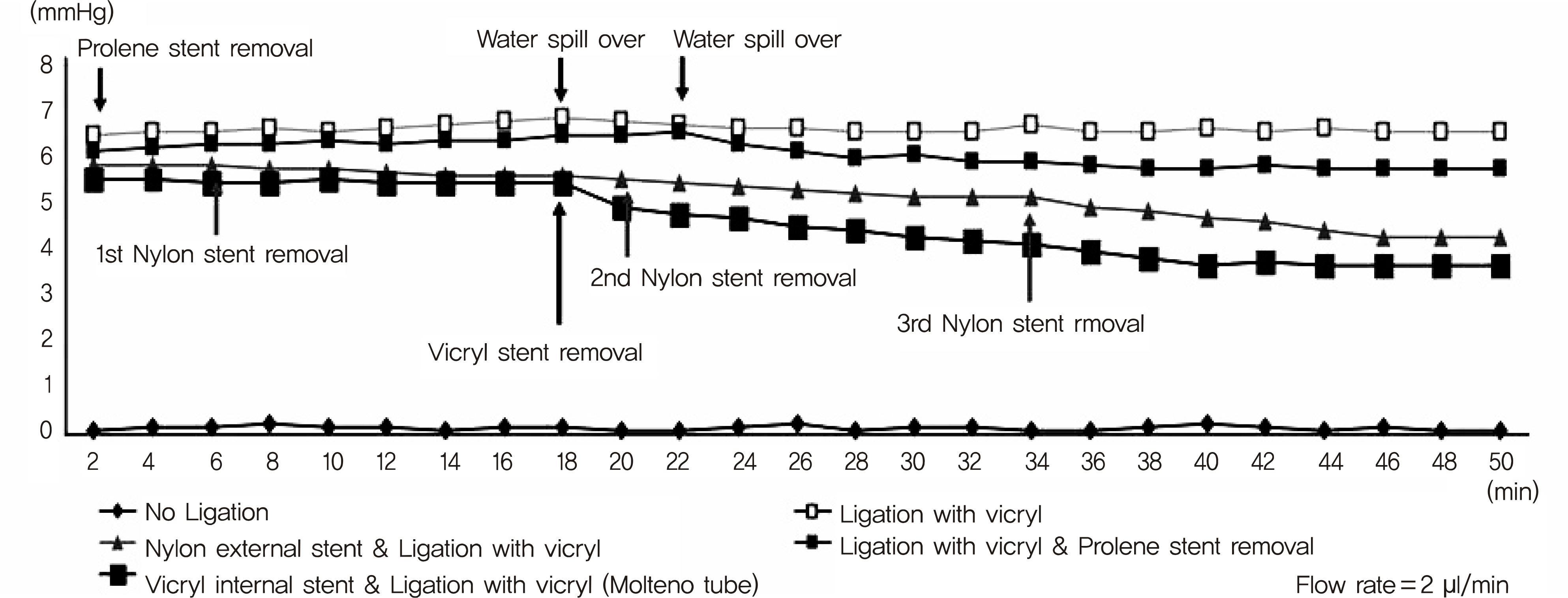
Figure 4. The measurement of flow resistance in Ahmed and Molteno implant using various tube ligation methods.
Reference
-
References
1. el-Sayyad F, el-Maghraby A, Helal M, Amayem A. The use of re-leasable sutures in Molteno glaucoma implant procedures to reduce postoperative hypotony. Ophthalmic Surg. 1991; 22:82–4.
Article2. Lee HJ, Choi KR. Clinical experience with the ahmed glaucoma valve implant in refractory glaucoma. J Korean Ophthalmol Soc. 2006; 47:933–40.3. Kim DH, Park CK, Ahn MD. Clinical results of ahmed valve implantation in the aspects of complications. J Korean Ophthalmol Soc. 2003; 44:888–95.4. Lee SH, Ma KT, Hong YJ. Outcome of ahmed valve implantation in refractory glaucoma. J Korean Ophthalmol Soc. 2007; 48:83–90.5. Zorab A. The reduction of tension in chronic glaucoma. Ophthalmoscope. 1912; 10:258–61.6. Molteno AC. New implant for drainage in glaucoma. Clinical trial. Br J Ophthalmol. 1969; 53:606–15.
Article7. Lloyd MA, Baerveldt G, Heuer DK, et al. Initial clinical experience with the baerveldt implant in complicated glaucomas. Ophthalmology. 1994; 101:640–50.
Article8. Schocket SS, Lakhanpal V, Richards RD. Anterior chamber tube shunt to an encircling band in the treatment of neovascular glaucoma. Ophthalmology. 1982; 89:1188–94.
Article9. Krupin T, Podos SM, Becker B, Newkirk JB. Valve implants in filtering surgery. Am J Ophthalmol. 1976; 81:232–5.
Article10. Joseph NH, Sherwood MB, Trantas G, et al. A one-piece drainage system for glaucoma surgery. Trans Ophthalmol Soc U K. 1986; 105:657–64.11. Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the ahmed glaucoma valve implant. Am J Ophthalmol. 1995; 120:23–31.
Article12. Schwartz AL, Anderson DR. Trabecular surgery. Arch Ophthalmol. 1974; 92:134–8.
Article13. Allen RC, Bellows AR, Hutchinson BT, Murphy SD. Filtration surgery in the treatment of neovascular glaucoma. Ophthalmology. 1982; 89:1181–7.
Article14. Englert JA, Freedman SF, Cox TA. The Ahmed valve in refractory pediatric glaucoma. Am J Ophthalmol. 1999; 127:34–42.
Article15. Huang MC, Netland PA, Coleman AL, et al. Intermediate-term clinical experience with the Ahmed Glaucoma Valve implant. Am J Ophthalmol. 1999; 127:27–33.16. Ayyala RS, Zurakowski D, Smith JA, et al. A clinical study of the Ahmed glaucoma valve implant in advanced glaucoma. Ophthalmology. 1998; 105:1968–76.17. Coleman AL, Smyth RJ, Wilson MR, Tam M. Initial clinical experience with the Ahmed Glaucoma Valve implant in pediatric patients. Arch Ophthalmol. 1997; 115:186–91.
Article18. Kee C. Prevention of early postoperative hypotony by partial ligation of silicone tube in Ahmed glaucoma valve implantation. J Glaucoma. 2001; 10:466–9.
Article19. Lee J, Kim Y, Kee C. The effect of partial occlusion of silicone tube on opening and closing pressure and flow rate. J Korean Ophthalmol Soc. 2000; 41:2709–14.20. Lee JJ, Park KH, Kim DM, Kim TW. Clinical outcomes of ahmed glaucoma valve implantation using tube ligation and removable external stents. Korean J Ophthalmol. 2009; 23:86–92.
Article21. Prata JA Jr, Mérmoud A, LaBree L, Minckler DS. In vitro and in vivo flow characteristics of glaucoma drainage implants. Ophthalmology. 1995; 102:894–904.
Article22. Francis BA, Cortes A, Chen J, Alvarado JA. Characteristics of glaucoma drainage implants during dynamic and steady-state flow conditions. Ophthalmology. 1998; 105:1708–14.
Article23. Topouzis F, Coleman AL, Choplin N, et al. Follow-up of the origi-nal cohort with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1999; 128:198–204.24. Krupin T, Ritch R, Camras CB, et al. A long Krupin-Denver valve implant attached to a 180 degrees scleral explants for glaucoma surgery. Ophthalmology. 1988; 95:1174–80.25. Huh KC, Kee CW. A clinical analysis of the ahmed glaucoma valve implant with or without partial ligation of silicone tube. J Korean Ophthalmol Soc. 2000; 41:2611–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ligation of Thoracic Duct Via Extrapleural Approach for the Treatment of Chylothorax: Report of 1 case
- Experimental Study for Measurement of Ureteral Compliance in Rat
- A Case of Total Vitrectomy in Aphakic Refractory Glaucoma with Prior Keratoplasty after Ahmed Glaucoma Valve Implantation
- The Comparison of Endoscopic Variceal Band Ligation (EVL) with and without Over Tube
- Resistance of Fluid Flow within the Nasolacrimal Duct
