Clinicopathological Study of Lacrimal Sac Dacryolith in Patients Treated for Nasolacrimal Duct Obstruction
- Affiliations
-
- 1Department of Ophthalmology, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea. eye@cha.ac.kr
- 2Department of Pathology, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea.
- KMID: 2213827
- DOI: http://doi.org/10.3341/jkos.2016.57.1.6
Abstract
- PURPOSE
To evaluate the correlation between clinical manifestation of patients with nasolacrimal duct obstruction and pathological characteristics of lacrimal sac and dacryolith found during endoscopic dacryocystorhinostomy.
METHODS
This retrospective study included 158 patients (189 eyes) who received endoscopic dacryocystorhinostomy. We defined lacrimal dacryolith by gross discovery in the lacrimal sac during surgery or findings during pathological examination as dacryolith or calcification, including size and distribution in pathology slides. We correlated the relationship between the patients' clinical manifestations, surgical results, lacrimal sac's pathological findings including calcification, inflammation and fibrosis, and pathological findings of lacrimal sac dacryolith.
RESULTS
Dacryolith was found in 61 eyes (32.3%) and among them, grossly found in 13 eyes (6.9%). Dacryolith's filling defect on dacryocystography was found in 17 eyes (9.0%) and based on grossly found dacryolith, dacryocystography's sensitivity and specificity were 58.8% and 1.7%, respectively. The average size of dacryolith was 0.3 +/- 0.8 mm2 with an average distribution of 20.1 +/- 17.9%. Distribution of dacryolith and the proportions of inflammatory cells and fibrosis in the lacrimal sac were negatively correlated (p < 0.05). The size of dacryolith and the proportions of fibrosis in the lacrimal sac were also negatively correlated (p = 0.008). In cases where the proportion of calcification in pathology slides was over 50%, the duration of symptoms in the calcification-dominant group was shorter than in other groups (p = 0.006). The success rates of endoscopic dacryocystorhinostomy with dacryolith and without dacryolith were 91.8% and 80.5%, respectively (p = 0.046).
CONCLUSIONS
The patients with lacrimal sac dacryolith in nasolacrimal duct obstruction showed shorter duration of symptoms, lower fibrosis of lacrimal sac, and higher surgical success rates than the other cases. Therefore, additional research may be necessary to determine the mechanism of dacryolith formation and early treatment in nasolacrimal duct obstruction with lacrimal sac dacryolith.
Keyword
MeSH Terms
Figure
-
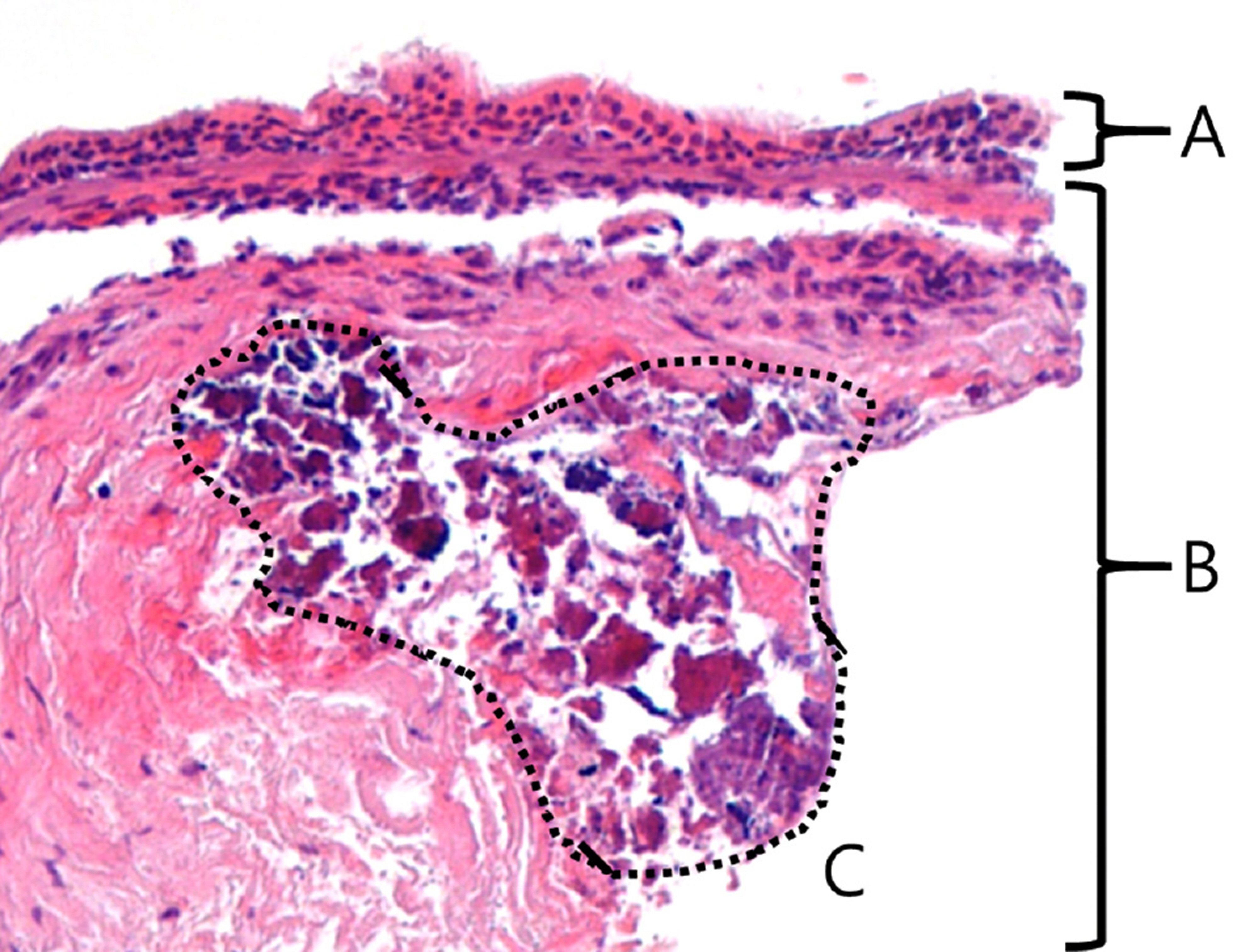
Figure 1. Histopathologic findings of calcification in lacrimal sac dacryolith. (A) Lacrimal sac epithelium. (B) Submucosa layer. (C) Calcification (Hematoxylin & Eosin stain, ×100).

Figure 2. Measurement of size for lacrimal sac dacryolith. Size (mm2) = longest length (A) × shortest length (B) of da-cryolith (Hematoxylin & Eosin stain, ×100).

Figure 3. The major pathologic findings of the lacrimal sac. (A) Calcification-dominant lacrimal sac (Hematoxylin & Eosin stain, ×100). (B) Inflammation-dominant lacrimal sac (Hematoxylin & Eosin stain, ×100). (C) Fibrosis-dominant lacrimal sac (Hematoxylin & Eosin stain, ×100).

Figure 4. Histopathologic analysis of lacrimal sac based on the severity of fibrosis and inflammation. (A) Indicator for measurement of tissue’s occupying ratio (arrow, 150 μ m-sized, HE stain, ×100). (B) Inflammatory portion of lacrimal sac (surrounded by dash-ed-line, HE stain, ×100; Black solid line = 150 μ m). (C) Fibrotic portion of lacrimal sac (surrounded by dashed-line, HE stain, ×100; Black solid line = 150 μ m). HE = Hematoxylin & Eosin.

Figure 5. The results of dacryocystography in patients with dacryolith. (A) Filling defect of lacrimal sac in dacryocystography’s finding. (B) Nasolacrimal duct stenosis without filling defect of the lacrimal sac.
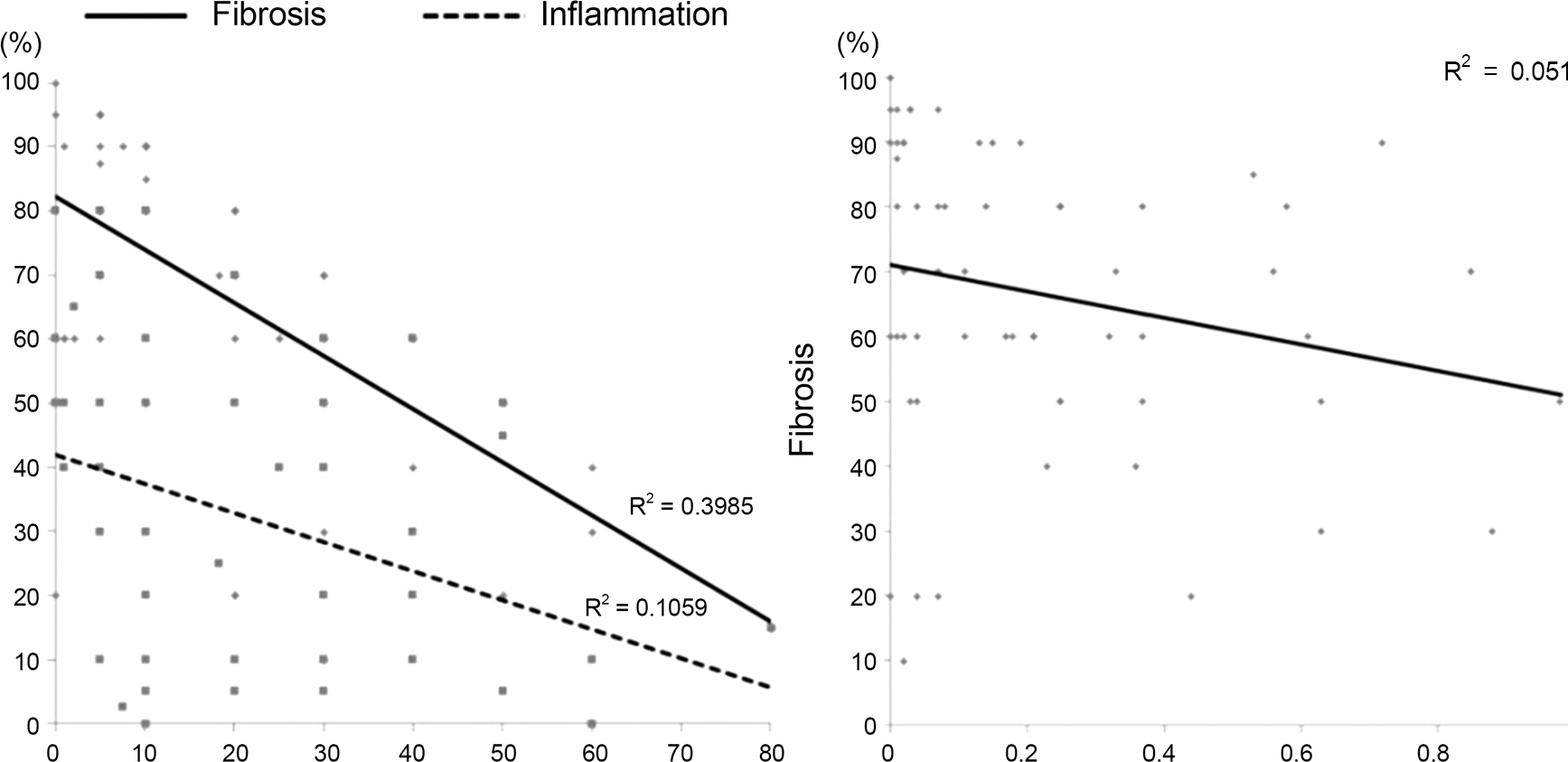
Figure 6. The results of correlation analysis between pathologic properties of dacryolith and the lacrimal sac.
Cited by 1 articles
-
Clinical Efficacy of Lacrimal Endoscopy Assisted Silicone Tube Intubation in Patients with Nasolacrimal Duct Obstruction
Sang Min Lee, Sok Joong Chung, Helen Lew
J Korean Ophthalmol Soc. 2018;59(6):582-588. doi: 10.3341/jkos.2018.59.6.582.
Reference
-
References
1. Berlin AJ, Rath R, Rich L. Lacrimal system dacryoliths. Ophthalmic Surg. 1980; 11:435–6.2. Rosen WJ, Rose GE. Intranasal passage of dacryoliths. Br J Ophthalmol. 2000; 84:799–800.
Article3. Yazici B, Hammad AM, Meyer DR. Lacrimal sac dacryoliths: pre-dictive factors and clinical characteristics. Ophthalmology. 2001; 108:1308–12.4. Halborg J, Prause JU, Toft PB. . Stones in the lacrimal gland: a rare condition. Acta Ophthalmol. 2009; 87:672–5.
Article5. Repp DJ, Burkat CN, Lucarelli MJ. Lacrimal excretory system concretions: canalicular and lacrimal sac. Ophthalmology. 2009; 116:2230–5.
Article6. Herzig S, Hurwitz JJ. Lacrimal sac calculi. Can J Ophthalmol. 1979; 14:17–20.7. Hawes MJ. The dacryolithiasis syndrome. Ophthal Plast Reconstr Surg. 1988; 4:87–90.
Article8. Wilkins RB, Pressly JP. Diagnosis and incidence of lacrimal calculi. Ophthalmic Surg. 1980; 11:787–9.9. Jones LT. Tear-sac foreign bodies. Am J Ophthalmol. 1965; 60:111–3.
Article10. Andreou P, Rose GE. Clinical presentation of patients with dacryolithiasis. Ophthalmology. 2002; 109:1573–4.
Article11. Komínek P, Č ervenka S, Zeleník K. . Lacrimal sac dacryolith (76 cases): a predictive factor for successful endonasal dacryocys-torhinostomy? Eur Arch Otorhinolaryngol. 2014; 271:1595–9.12. Anderson NG, Wojno TH, Grossniklaus HE. Clinicopathologic findings from lacrimal sac biopsy specimens obtained during dacryocystorhinostomy. Ophthal Plast Reconstr Surg. 2003; 19:173–6.
Article13. Tucker N, Chow D, Stockl F. . Clinically suspected primary ac-quired nasolacrimal duct obstruction: clinicopathologic review of 150 patients. Ophthalmology. 1997; 104:1882–6.14. Lee SH, Lew H, Sim JY. Pathologic features of lacrimal sac muco-sa in primary acquired nasolacrimal duct obstruction patients. J Korean Ophthalmol Soc. 2004; 45:173–9.15. Park DI, Lew H, Lee SY. Tear meniscus measurement in nasolacri-mal duct obstruction patients with Fourier-domain optical coher-ence tomography: novel three-point capture method. Acta Ophthalmol. 2012; 90:783–7.
Article16. Kim CH, Lew H, Yun YS. Correspondence among the canaliculus irrigation test, dacryocystography and Jones test in the epiphora patients. J Korean Ophthalmol Soc. 2007; 48:1017–22.
Article17. Orhan M, Onerci M, Dayanir V. . Lacrimal sac dacryolith: a study with atomic absorption spectrophotometry and scanning electron microscopy. Eur J Ophthalmol. 1996; 6:478–80.
Article18. Iliadelis E, Karabatakis V, Sofoniou M. Dacryoliths in chronic dacryocystitis and their composition (spectrophotometric analysis). Eur J Ophthalmol. 1999; 9:266–8.
Article19. Rhim WI, Lew H, Yun YS, Ahn HJ. A case of morphological and chemical analysis of recurrent dacryoliths after dacryocystorhinostomy. J Korean Ophthalmol Soc. 2002; 43:1128–32.20. Lee-Wing MW, Ashenhurst ME. Clinicopathologic analysis of 166 patients with primary acquired nasolacrimal duct obstruction. Ophthalmology. 2001; 108:2038–40.
Article21. Paulsen FP, Thale AB, Maune S, Tillmann BN. New insights into the pathophysiology of primary acquired dacryostenosis. Oph- thalmology. 2001; 108:2329–36.
Article22. Salour H, Hatami MM, Parvin M. . Clinicopathological study of lacrimal sac specimens obtained during DCR. Orbit. 2010; 29:250–3.
Article23. Ozer O, Eskiizmir G, Unlü H. . Chronic inflammation: a poor prognostic factor for endoscopic dacryocystorhinostomy. Eur Arch Otorhinolaryngol. 2012; 269:839–45.
Article24. Nixon J, Birchall IW, Virjee J. The role of dacryocystography in the management of patients with epiphora. Br J Radiol. 1990; 63:337–9.
Article25. Milder B, Demorest BH. Dacryocystography. I. The normal lac-rimal apparatus. AMA Arch Ophthalmol. 1954; 51:180–95.26. Ewing AE. Roentgen ray demonstration of the lacrimal abscess cavity. Am J Ophthalmol. 1909; 24:1–4.27. Marcet MM, Kuk AK, Phelps PO. Evidence-based review of surgi-cal practices in endoscopic endonasal dacryocystorhinostomy for primary acquired nasolacrimal duct obstruction and other new indications. Curr Opin Ophthalmol. 2014; 25:443–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Nasolacrimal Duct Obstruction Caused by a Lacrimal Sac Retention Cyst
- Results with Silicone Stent in Lacrimal Drainage System
- The Role of Dacryocystography in Evaluation of Nasolacrimal Duct Obstruction
- Result of Partial Nasolacrimal Duct Obstruction After Silicone Tube Intubation
- Nasolacrimal Duct Obstruction Following Midfacial Autologous Fat Injection
