A Case of Amantadine-Induced Corneal Edema
- Affiliations
-
- 1Department of Ophthalmology, Yeungnam University College of Medicine, Daegu, Korea. sbummlee@med.yu.ac.kr
- 2Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2212374
- DOI: http://doi.org/10.3341/jkos.2009.50.6.936
Abstract
-
PURPOSE: To report a rare case of corneal edema caused by amantadine.
CASE SUMMARY
A 35-year-old man was diagnosed with hypoxic brain damage caused by ventricular fibrillation. The patient showed Parkinsonism and was started on treatment with amantadine. Thirty-seven months after the commencement of amantadine treatment, the patient suffered a corneal ulcer in his right eye, which healed with opacity and thinning after medical treatment. After healing, slit-lamp examination revealed a bilateral, epithelial and stromal edema without obvious guttae and keratic precipitates. The corneal edema did not improve with topical treatment of 5% NaCl and 0.02% fluorometholone in both eyes. Three months after leaving the hospital, the patient's corrected visual acuity decreased to 0.2 (-2.0 Dsph -0.5 Dcyl Ax 90) in the right eye and 0.4 (-0.75 Dsph -2.0 Dcyl Ax 90) in the left eye. Amantadine medication was discontinued after discussion with the patient's neurologist. At the 1-month follow-up, corneal examination revealed resolution of the epithelial and stromal edema in both eyes. Corrected visual acuity was improved to 0.5 (-1.5 Dsph) in the right eye and 0.7 (-1.0 Dsph -1.0 Dcyl Ax 90) in the left eye.
CONCLUSIONS
In cases of corneal edema without an obvious causative disease, the patient's systemic medication list must be reviewed and amantadine should be considered as a possible cause.
Keyword
MeSH Terms
Figure
-

Figure 1. At 15 days after discontinuation of amantadine medication, the patient showed central corneal opacity and thinning with decreased epithelial and stromal edema in the right eye, and mild epithelial and stromal edema with minimal Descemet's membrane folds in the left eye. Ultrasound pachymetry revealed a central corneal thickness of 581 μm in the right eye and 630 μm in the left eye.

Figure 2. Specular photomicrographs of both eyes showed marked enlargement of the corneal endothelium and decrease of the corneal endothelial cell density at 15 days after discontinuation of amantadine medication. Cell density, coefficient of variation, and frequency of hexagons are 863±563 cells/mm2, 0.480, and 48.0% in the right eye, and 919±490 cells/mm2, 0.450, and 49.0% in the left eye, respectively.
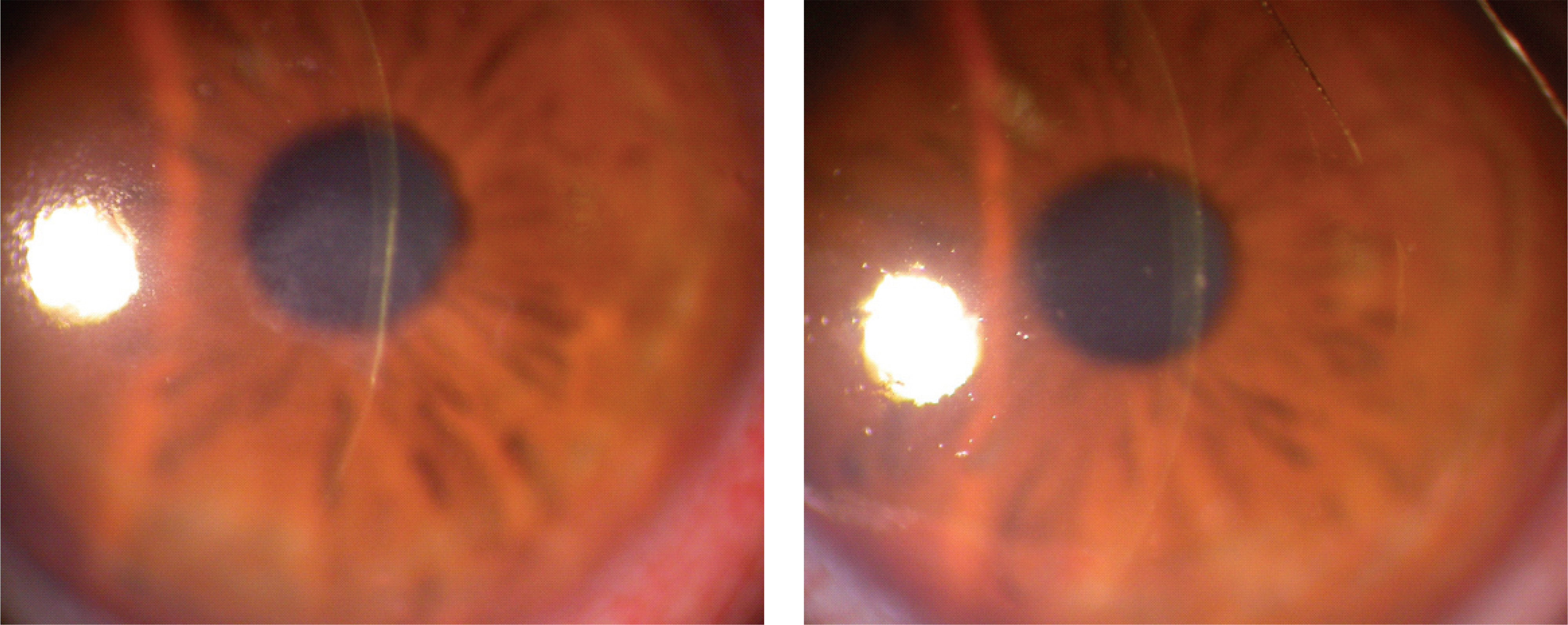
Figure 3. At 1 month after discontinuation of amantadine medication, the patient showed resolution of epithelial and stromal edema of the cornea in both eyes with only central opacity and thinning in the right eye. Ultrasound pachymetry revealed a central corneal thickness of 421 μm in the right eye and 495 μm in the left eye.

Figure 4. At 1 month after discontinuation of amantadine medication, cell density, coefficient of variation, and frequency of hexagons of specular photomicrographs are 876±537 cells/mm2, 0.470, and 49.0% in the right eye, and 788±529 cells/mm2, 0.410, and 46.0% in the left eye, respectively.
Reference
-
References
1. Offret H, Labetoulle M, Offret O. Corneal edema and systemic NSAIDS. J Fr Ophthalmol. 2007; 30:e14.2. Platt LW. Bilateral peripheral corneal edema after cefaclor therapy. Arch Ophthalmol. 1990; 108:175.
Article3. Oshika T, Itotagawa K, Sawa M. Severe corneal edema after prolonged use of psychotropic agents. Cornea. 1991; 10:354–7.
Article4. Fraunfelder FT, Fraunfelder FW. Drug-induced ocular side effects. 5th ed.Boston: Butterworth-Heinemann;2001. p. 421–2.5. Blanchard DL. Amantadine caused corneal edema. Cornea. 1990; 9:181.
Article6. Amantadine. Physician's Desk References. 57th ed.Montvale, NJ: Thompson healthcare;2003. p. 1213–5.7. Hughes B, Feiz V, Flynn SB, Brodsky MC. Reversible amantadine-induced corneal edema in adolescent. Cornea. 2004; 23:823–4.8. Kubo SI, Iwatake A, Ebihara N, et al. Visual impairment in Parkinson's disease treated with amantadine: case report and review of the literature. Parkinsonism Relat Disord. 2007; 14:166–9.
Article9. Jeng BH, Galor A, Lee MS, et al. Amantadine-associated corneal edema potentially irreversible even after cessation of the medication. Ophthalmology. 2008; 115:1540–4.10. French DD, Margo CE. Postmarketing surveillance of corneal edema, Fuchs dystrophy, and amantadine use in the Veterans Health Administration. Cornea. 2007; 26:1087–9.
Article11. Kornhuber J, Weller M, Schoppmeyer K, et al. Amantadine and memantine are NMDA receptor antagonist with neuroprotective properties. J Neural Transm Supple. 1994; 43:91–104.12. Fraunfelder FT, Meyer SM. Amantadine and corneal deposits. Am J Ophthalmol. 1990; 110:96–7.
Article13. Chang KC, Kim MK, Wee WR, Lee JH. Corneal endothelial dysfunction associated with amantadine toxicity. Cornea. 2008; 27:1182–85.
Article14. Schwab RS, England Jr AC, Poskanzer DC, Young RR. Amantadine in the treatment of Parkinson's disease. JAMA. 1969; 208:1168–70.
Article15. Krachmer JH, Mannis MJ, Holland EJ. Cornea. 2nd ed. 1. Philadelphia: Elsevier Inc.;2005. p. 360.16. Waring GO Ⅲ. Posterior collagenous layer of the cornea: ultrastructural classification of abnormal collagenous tissue posterior to Descemet's membrane in 30 cases. Arch Ophthalmol. 1982; 100:122–34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Irreversible Corneal Endothelial Damage Associated with Amantadine Use
- A double-blind study of amantadine sulfate versus benztropine mesylate in antipsychotic drug-induced extrapyramidal symptoms
- Bilateral Pleural Effusion Possibly Related to Amantadine
- The Effect of Corneal Edema on Corneal Topography
- Therapeutic Uses of T-lens(Soflens(R)) in Corneal Diseases
