Orthodontic treatment for maxillary anterior pathologic tooth migration by periodontitis using clear aligner
- Affiliations
-
- 1Department of Periodontology, Chosun University College of Dentistry, Gwangju, Korea. aime-82@daum.net
- KMID: 2212134
- DOI: http://doi.org/10.5051/jpis.2011.41.1.44
Abstract
- PURPOSE
Pathologic tooth migration (PTM) is a tooth displacement which is derived from imbalance of tooth retention force and is dominantly found out in maxillary anterior area. PTM in maxillary anterior area was tried to corrected with periodontal treatment and a clear aligner in this study and the result was evaluated clinically and radiographically.
METHODS
For the treatment of a patient with chronic periodontal disease accompanied by maxillary anterior pathologic tooth migration, clear aligner was applied to move teeth after a series of case-related periodontal therapy. Clinically, probing depth, gingival recession, clinical attachment level and mobility were measured pre- and post-treatment, and radiographic examination was performed as well.
RESULTS
Clinically, we found the decrease of the probing depth, gingival recession, clinical attachment level and mobility. And we could also acknowledge the reduction of vertical and horizontal dimension on infrabony defect radiographically. However, it is still controversial if there was an actual bone filling.
CONCLUSIONS
Clear aligner is an effective appliance to move teeth since it costs little in terms of expense and time. In addition, it wraps whole crowns, providing advantages to deal with crowding, spacing, and size of arch. In short, clear aligner could be a useful treatment option for PTM patient, since it provides decreased probing depth, gingival recession, clinical attachment level, mobility and esthetical restoration.
MeSH Terms
Figure
-
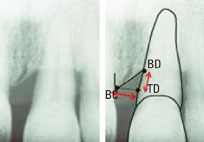
Figure 1 Radiographic measurement. BC: horizontal distance from bone crest, BD: the most apical point of the bone defect, TD: vertical distance between the horizontal projection of the bone crest on the root surface, TD-BD: vertical dimension, BC-TD: horizontal dimension.
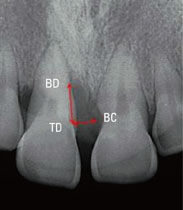
Figure 2 Radiographic examination at first visit. BC: horizontal distance from bone crest, BD: the most apical point of the bone defect, TD: vertical distance between the horizontal projection of the bone crest on the root surface, TD-BD: vertical dimension, BC-TD: horizontal dimension.

Figure 3 Pre-periodontal treatment (clinical photograph of the front view).

Figure 4 Pre-periodontal treatment (clinical photograph of the occlusal plane view).

Figure 5 Making the appliance (photograph of the cast from the front side).

Figure 6 Making the appliance (photograph of the cast viewed from the occlusal plane).

Figure 7 Clear aligner.

Figure 8 Three weeks after initial visit (clinical photograph of the front side).

Figure 9 Three weeks after initial visit (clinical photograph of the occlusal plane).

Figure 10 Appliance fabrication after 3 weeks (photograph of the cast from the front side).

Figure 11 Appliance fabrication after 3 weeks (photograph of the cast from the occlusal plane).

Figure 12 Six weeks after initial visit (clinical photograph of the front side).

Figure 13 Six weeks after initial visit (clinical photograph of the occlusal plane).

Figure 14 Post-treatment. Radiography. BD: the most apical point of the bone defect, TD: vertical distance between the horizontal projection of the bone crest on the root surface, BC: horizontal distance from bone crest, TD-BD: vertical dimension, BC-TD: horizontal dimension.

Figure 15 Retention.

Figure 16 Radiographic examination at first visit. BC: horizontal distance from bone crest, BD: the most apical point of the bone defect, TD: vertical distance between the horizontal projection of the bone crest on the root surface, TD-BD: vertical dimension, BC-TD: horizontal dimension.

Figure 17 Pre-periodontal treatment (clinical photograph at the front side view).

Figure 18 Pre-periodontal treatment (clinical photograph at the occlusal plane).

Figure 19 Appliance implementation (clinical photograph of the front side).

Figure 20 Appliance implementation (clinical photograph of the occlusal plane).

Figure 21 Three weeks after initial visit (clinical photograph of the front side).

Figure 22 Three weeks after initial visit (clinical photograph of the occlusal plane).

Figure 23 Six weeks after initial visit (clinical photograph of the front side).

Figure 24 Six weeks after initial visit (clinical photograph of the occlusal plane).

Figure 25 After prosthetic treatment (clinical photograph of the front side).

Figure 26 After prosthetic treatment (clinical photograph of the occlusal plane).

Figure 27 Post-treatment. Radiography. BC: horizontal distance from bone crest, BD: the most apical point of the bone defect, TD: vertical distance between the horizontal projection of the bone crest on the root surface, TD-BD: vertical dimension, BC-TD: horizontal dimension.

Figure 28 Radiographic examination at first visit.

Figure 29 Pre-periodontal treatment (clinical photograph of the front side).

Figure 30 Pre-periodontal treatment (clinical photograph of the occlusal plane).

Figure 31 Three weeks after initial visit (clinical photograph of the front side).

Figure 32 Three weeks after initial visit (clinical photograph of the occlusal plane).

Figure 33 Six weeks after initial visit (clinical photograph of the front side).

Figure 34 Six weeks after initial visit (clinical photograph of the occlusal plane).

Figure 35 Retention.
Reference
-
1. Chasens AI. Periodontal disease, pathologic tooth migration and adult orthodontics. N Y J Dent. 1979. 49:40–43.2. Martinez-Canut P, Carrasquer A, Magán R, Lorca A. A study on factors associated with pathologic tooth migration. J Clin Periodontol. 1997. 24:492–497.
Article3. Brunsvold MA. Pathologic tooth migration. J Periodontol. 2005. 76:859–866.
Article4. Sutton PR, Graze HR. The blood-vessel thrust theory of tooth eruption and migration. Med Hypotheses. 1985. 18:289–295.
Article5. Remensnyder O. A gum-massaging appliance in the treatment of pyorrhea. Dent Cosmos. 1926. 28:381–384.6. Kesling HD. The philosophy of the tooth positioning appliance. Am J Orthod Oral Surg. 1945. 31:297–304.
Article7. Kim TW. Principle and clinical application of clear aligner. 2005. Seoul: Myungmun Publishing Co;60–76.8. Kim TW. Principle and clinical application of clear aligner. 2005. Seoul: Myungmun Publishing Co;18–47.9. Ericsson I, Thilander B, Lindhe J. Periodontal conditions after orthodontic tooth movements in the dog. Angle Orthod. 1978. 48:210–218.10. Wennström JL, Stokland BL, Nyman S, Thilander B. Periodontal tissue response to orthodontic movement of teeth with infrabony pockets. Am J Orthod Dentofacial Orthop. 1993. 103:313–319.
Article11. Lindhe J, Karring T, Lang NP. Clinical periodontology and implant dentistry. 2003. 4th ed. Oxford: Blackwell;752–754.12. Corrente G, Abundo R, Re S, Cardaropoli D, Cardaropoli G. Orthodontic movement into infrabony defects in patients with advanced periodontal disease: a clinical and radiological study. J Periodontol. 2003. 74:1104–1109.
Article13. Melsen B, Agerbaek N, Markenstam G. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofacial Orthop. 1989. 96:232–241.
Article14. Re S, Corrente G, Abundo R, Cardaropoli D. Orthodontic movement into bone defects augmented with bovine bone mineral and fibrin sealer: a reentry case report. Int J Periodontics Restorative Dent. 2002. 22:138–145.15. Proffit WR. Equilibrium theory revisited: factors influencing position of the teeth. Angle Orthod. 1978. 48:175–186.16. Dahl EH, Zachrisson BU. Long-term experience with direct-bonded lingual retainers. J Clin Orthod. 1991. 25:619–630.17. Nyman S, Karring T, Bergenholtz G. Bone regeneration in alveolar bone dehiscences produced by jiggling forces. J Periodontal Res. 1982. 17:316–322.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intrusion of the extruded maxillary central incisor using skeletal anchorage system and unilateral segmental intrusion arch
- Full mouth rehabilitation on the patient with maxillary anterior diastema and posterior bite collapse with orthodontic treatment
- Orthodontic treatment using indirect bonding technique in periodontitis
- Combined periodontal regenerative and prosthetic treatment of pathologic migration of anterior teeth
- Orthodontic treatment with clear aligners for a patient with chronic periodontitis
