J Korean Surg Soc.
2010 Nov;79(5):386-392. 10.4174/jkss.2010.79.5.386.
Results of Simultaneous Hybrid Operation in Multi-level Arterial Occlusive Disease
- Affiliations
-
- 1Division of Vascular/Endovascular Surgery, Department of Surgery, Daegu Catholic University Medical Center, Daegu, Korea. winderror@yahoo.co.kr
- KMID: 2212047
- DOI: http://doi.org/10.4174/jkss.2010.79.5.386
Abstract
- PURPOSE
Hybrid procedure in lower extremity arterial disease is composed of open bypass and endovascular treatment. For proximal inflow bypass operations for distal lesions used to be performed 1 or 2 weeks after endovascular therapy. Since Aug 2005, all hybrid operations have been performed simultaneously in the operation room in our center. In this study, we compared the results of the staged hybrid operations with those of simultaneous procedures.
METHODS
From Jan 1999 to Dec 2009, 115 endovascular treatments and 139 bypass operations were performed. 44 bypasses were performed 1 day to 14 days after angioplasty in inflow lesions (group I) and 95 bypasses were performed simultaneously in the operation room with mobile fluoroscopy (group II). In both groups, inflow procedures included 3 femoral balloon angioplasties, 3 femoral stents, 24 iliac balloon angioplasties and 85 iliac stents. Bypass operations were composed of 39 femorofemoral and 102 infrainguinal bypasses including 60 femoropopliteal and 42 other bypasses.
RESULTS
The 3-year patency rate of bypass graft is 71.5%. There is no difference in either group. But in endovascular treatment lesion, the 3-year patency rate is 80% and that of the simultaneous group is higher than that of the staged group (P<0.05).
CONCLUSION
Hybrid operation is a less invasive therapy for revascularization in multilevel peripheral arterial occlusive disease. With development of endovascular therapy, simultaneous hybrid operations become more efficient.
Figure
-
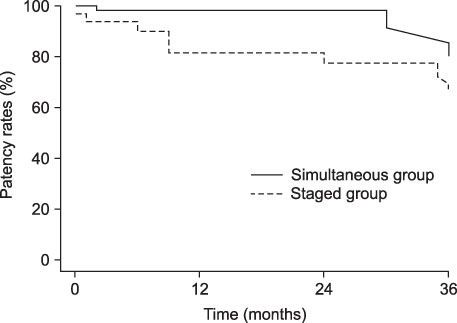
Fig. 1 Comparison of 3-year cumulative primary patency rates in endovascular treatment for iliac lesion between staged and simultaneous group.

Fig. 2 Comparison of 3-year cumulative primary patency rates in femoropopliteal bypass grafts between staged and simultaneous group.
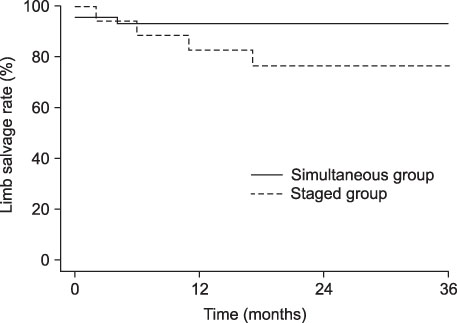
Fig. 3 Comparison of 3-year limb salvage rates between staged and simultaneous group.

Fig. 4 Wound hematoma due to previous puncture injury (black arrow).
Cited by 1 articles
-
Multiple drug-coated balloons can be used effectively for peripheral arterial disease including long femoropopliteal lesions
Wongong Chu, Dong Hyun Kim, Sukyung Kwon, Je-hyung Park, Hyuk Jae Jung, Sang Su Lee
Ann Surg Treat Res. 2021;101(2):120-128. doi: 10.4174/astr.2021.101.2.120.
Reference
-
1. Chiu KW, Davies RS, Nightingale PG, Bradbury AW, Adam DJ. Review of direct anatomical open surgical management of atherosclerotic aorto-iliac occlusive disease. Eur J Vasc Endovasc Surg. 2010. 39:460–471.2. Porter JM, Eidemiller LR, Dotter CT, Rosch J, Vetto RM. Combined arterial dilatation and femorofemoral bypass for limb salvage. Surg Gynecol Obstet. 1973. 137:409–412.3. Walker PJ, Harris JP, May J. Combined percutaneous transluminal angioplasty and extraanatomic bypass for symptomatic unilateral iliac artery occlusion with contralateral iliac artery stenosis. Ann Vasc Surg. 1991. 5:209–217.4. Pfeiffer RB Jr, String ST. Adjunctive use of the balloon dilatation catheter during vascular reconstructive procedures. J Vasc Surg. 1986. 3:841–845.5. Corey CJ, Bush HL Jr, Widrich WC, Nabseth DC. Combined operative angiodilation and arterial reconstruction for limb salvage. Arch Surg. 1983. 118:1289–1292.6. Vetto RM. The treatment of unilateral iliac artery obstruction with a transabdominal, subcutaneous, femorofemoral graft. Surgery. 1962. 52:343–345.7. Aburahma AF, Robinson PA, Cook CC, Hopkins ES. Selecting patients for combined femorofemoral bypass grafting and iliac balloon angioplasty and stenting for bilateral iliac disease. J Vasc Surg. 2001. 33:S93–S99.8. Becker GJ, Katzen BT, Dake MD. Noncoronary angioplasty. Radiology. 1989. 170:921–940.9. Palmaz JC, Laborde JC, Rivera FJ, Encarnacion CE, Lutz JD, Moss JG. Stenting of the iliac arteries with the Palmaz stent: experience from a multicenter trial. Cardiovasc Intervent Radiol. 1992. 15:291–297.10. Tetteroo E, van der Graaf Y, Bosch JL, van Engelen AD, Hunink MG, Eikelboom BC, et al. Dutch Iliac Stent Trial Study Group. Randomised comparison of primary stent placement versus primary angioplasty followed by selective stent placement in patients with iliac-artery occlusive disease. Lancet. 1998. 351:1153–1159.11. Alpert JR, Ring EJ, Freiman DB, Oleaga JA, Gordon R, Berkowitz HD, et al. Balloon dilation of iliac stenosis with distal arterial surgery. Arch Surg. 1980. 115:715–717.12. Johansen K, Ricketts H, Wales LR, Morishima M. Combined arterial reconstruction and transluminal dilatation: therapeutic teamwork to combat vascular insufficiency. World J Surg. 1981. 5:653–658.13. Howell HS, Ingram CH, Parham AR, Miller IB, Harriss WF, Wood JL, et al. Transluminal angioplasty of the iliac artery combined with femorofemoral bypass. South Med J. 1983. 76:49–51.14. Melliere D, Cron J, Allaire E, Desgranges P, Becquemin JP. Indications and benefits of simultaneous endoluminal balloon angioplasty and open surgery during elective lower limb revascularization. Cardiovasc Surg. 1999. 7:242–246.15. Doubilet P, Abrams HL. The cost of underutilization. Percutaneous transluminal angioplasty for peripheral vascular disease. N Engl J Med. 1984. 310:95–102.16. Perler BA, Williams GM. Does donor iliac artery percutaneous transluminal angioplasty or stent placement influence the results of femorofemoral bypass? Analysis of 70 consecutive cases with long-term follow-up. J Vasc Surg. 1996. 24:363–370.17. Kwon SB, Park KH, Jung SJ, Choi DR, Joo DH, Lee HI, et al. Multi detector row computed tomography angiogram as the sole preoperative imaging for infrainguinal arterial surgery. J Korean Soc Vasc Surg. 2004. 20:47–51.18. Calligaro KD, Dougherty MJ, Patterson DE, Raviola CA, DeLaurentis DA. Value of an endovascular suite in the operating room. Ann Vasc Surg. 1998. 12:296–298.19. Whiteley MS, Ray-Chaudhuri SB, Galland RB. Changing patterns in aortoiliac reconstruction: a 7-year audit. Br J Surg. 1996. 83:1367–1369.20. Kashyap VS, Pavkov ML, Bena JF, Sarac TP, O'Hara PJ, Lyden SP, et al. The management of severe aortoiliac occlusive disease: endovascular therapy rivals open reconstruction. J Vasc Surg. 2008. 48:1451–1457.21. Nishibe T, Kondo Y, Dardik A, Muto A, Koizumi J, Nishibe M. Hybrid surgical and endovascular therapy in multifocal peripheral TASC D lesions: up to three-year follow-up. J Cardiovasc Surg (Torino). 2009. 50:493–499.22. Chang RW, Goodney PP, Baek JH, Nolan BW, Rzucidlo EM, Powell RJ. Long-term results of combined common femoral endarterectomy and iliac stenting/stent grafting for occlusive disease. J Vasc Surg. 2008. 48:362–367.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Lower Extremity Ischemia due to Multilevel Arterial Occlusive Disease (II)
- Clinical Characteristics of Lower Limb Ischemia due to Multi-Level Arterial Occlusive Disease
- Staged Hybrid Revascularization in Patients with Peripheral Arterial Occlusive Disease
- Acute Arterial Occlusive Disease
- Initial Experiences of Endovascular Surgery for Lower Extremity Arterial Occlusive Diseases in the Operation Room
