Outcomes of nonsurgical periodontal therapy in severe generalized aggressive periodontitis
- Affiliations
-
- 1Department of Periodontology, Faculty of Dental Medicine, Biostatistical, Clinical, and Epidemiological Research Laboratory, Faculty of Medicine and Pharmacy, Mohammed V Souissi University, Rabat, Morocco. amal.bouziane@gmail.com
- 2Department of Periodontology, Faculty of Dental Medicine, Mohammed V Souissi University, Rabat, Morocco.
- 3Biostatistical, Clinical, and Epidemiological Research Laboratory, Faculty of Medicine and Pharmacy, Mohammed V Souissi University, Rabat, Morocco.
- 4Department of Periodontology, Faculty of Dental Medicine, Mohammed V Souissi University, Rabat, Morocco.
- KMID: 2212014
- DOI: http://doi.org/10.5051/jpis.2014.44.4.201
Abstract
- PURPOSE
Aggressive periodontitis, especially in its severe form, was traditionally considered to have an unfavourable prognosis. It required a complex treatment and its stabilization was often achieved by surgical therapy. The aim of this study was to investigate the results of nonsurgical periodontal treatment in severe generalized forms of aggressive periodontitis.
METHODS
Patients with advanced generalized aggressive periodontitis were included in the study. Probing depth (PD) of pockets > or =7 mm and clinical attachment level (CAL) of sites with attachment loss > or =5 mm were measured at baseline before nonsurgical periodontal treatment, at re-evaluation, and after treatment. The following other parameters were recorded: resolution of inflammation and bone fill. We compared the baseline values with re-evaluation and posttreatment values using the Friedman test. The Wilcoxon test with the Bonferroni correction was used for both re-evaluation and posttreatment values.
RESULTS
Seven patients with 266 periodontal sites were examined. A significant difference was found between values, reported as medians with interquartile ranges, for PD at baseline (7.94 [7.33-8.19] mm) and both re-evaluation (4.33 [3.63-5.08] mm) and posttreatment (3.54 [3.33-4.11] mm) values (P=0.002). A significant difference was also found between values for CAL at baseline (9.02 [7.5-9.2] mm) and both re-evaluation (6.55 [6.30-6.87] mm) and posttreatment (6.45 [5.70-6.61] mm) (P=0.002). Inflammation was resolved and angular bone defects were repaired in all cases.
CONCLUSIONS
These therapeutic results suggest that this form of periodontitis could have positive outcomes after nonsurgical periodontal treatment. The reparative potential of tissue affected by severe aggressive periodontitis should encourage clinicians to save apparently hopeless teeth in cases of this form of periodontitis.
MeSH Terms
Figure
-

Figure 1 Initial state of one of the severe generalized aggressive periodontitis cases.

Figure 2 Severe angular alveolar bone loss and furcation defect degree II at 36. Probing depth: 3.3.13 (Buccal), 3.2.11 (Lingual).

Figure 3 Improved pocket depth at re-evaluation. Probing depth: 2.2.7 (Buccal), 2.2.6 (Lingual).

Figure 4 Stability of the lesion 5 years after the aetiological treatment. Probing depth: 3.2.2 (Buccal), lingual 3.3.3.
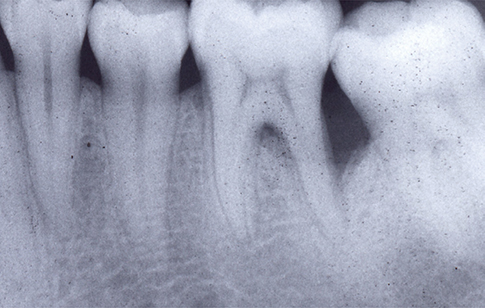
Figure 5 Radiographic improvement of the lesion.
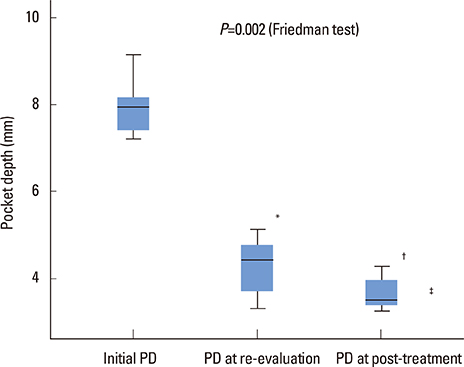
Figure 6 Diagram demonstrating changes in pocket depth in millimeters (median and quartiles) at baseline, re-evaluation, and posttreatment after using Friedman and Wilcoxon tests. *P=0.05, re-evaluation vs. initial. †P=0.05, posttreatment vs. initial. ‡P=0.12, re-evaluation vs. posttreatment. PD: probing depth.
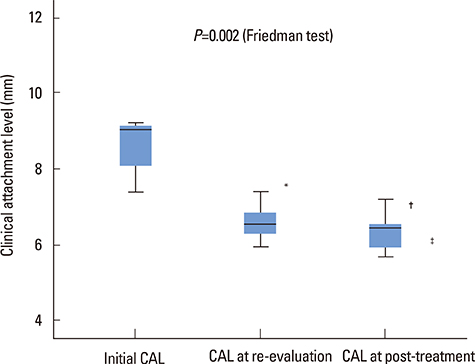
Figure 7 Diagram demonstrating changes in clinical attachment loss (CAL) in millimeters at baseline, at re-evaluation, and posttreatment after using Friedman and Wilcoxon tests. *P=0.05, re-evaluation vs. initial. †P=0.05, posttreatment vs. initial. ‡P=0.27, re-evaluation vs. posttreatment.
Reference
-
1. American Academy of Periodontology. Parameter on aggressive periodontitis. J Periodontol. 2000; 71:5 Suppl. 867–869.
Article2. Demmer RT, Papapanou PN. Epidemiologic patterns of chronic and aggressive periodontitis. Periodontol 2000. 2010; 53:28–44.
Article3. Haubek D, Ennibi OK, Poulsen K, Poulsen S, Benzarti N, Kilian M. Early-onset periodontitis in Morocco is associated with the highly leukotoxic clone of Actinobacillus actinomycetemcomitans. J Dent Res. 2001; 80:1580–1583.
Article4. Eickholz P, Kaltschmitt J, Berbig J, Reitmeir P, Pretzl B. Tooth loss after active periodontal therapy. 1: patient-related factors for risk, prognosis, and quality of outcome. J Clin Periodontol. 2008; 35:165–174.
Article5. Dubrez B, Baehni P, Cimasoni G. A case of localized juvenile periodontitis: treatment and 3 years follow-up with superimposable radiographs. J Clin Periodontol. 1996; 23:557–562.
Article6. Sewon LA. Rapid bony healing in localized juvenile periodontitis: a case report. Scand J Dent Res. 1993; 101:371–374.
Article7. Novak MJ, Stamatelakys C, Adair SM. Resolution of early lesions of juvenile periodontitis with tetracycline therapy alone: long-term observations of 4 cases. J Periodontol. 1991; 62:628–633.
Article8. Mattout P, Moskow BS, Fourel J. Repair potential in localized juvenile periodontitis: a case in point. J Periodontol. 1990; 61:653–660.
Article9. Moskow BS. Healing potential in periodontal lesions: localized juvenile periodontitis. J N J Dent Assoc. 1986; 57:45–51.10. Lindhe J, Liljenberg B. Treatment of localized juvenile periodontitis: results after 5 years. J Clin Periodontol. 1984; 11:399–410.
Article11. Buchmann R, Nunn ME, Van Dyke TE, Lange DE. Aggressive periodontitis: 5-year follow-up of treatment. J Periodontol. 2002; 73:675–683.12. Kamma JJ, Baehni PC. Five-year maintenance follow-up of early-onset periodontitis patients. J Clin Periodontol. 2003; 30:562–572.
Article13. Aimetti M, Romano F, Guzzi N, Carnevale G. One-stage full-mouth disinfection as a therapeutic approach for generalized aggressive periodontitis. J Periodontol. 2011; 82:845–853.
Article14. Aimetti M, Romano F, Guzzi N, Carnevale G. Full-mouth disinfection and systemic antimicrobial therapy in generalized aggressive periodontitis: a randomized, placebo-controlled trial. J Clin Periodontol. 2012; 39:284–294.
Article15. Griffiths GS, Ayob R, Guerrero A, Nibali L, Suvan J, Moles DR, et al. Amoxicillin and metronidazole as an adjunctive treatment in generalized aggressive periodontitis at initial therapy or re-treatment: a randomized controlled clinical trial. J Clin Periodontol. 2011; 38:43–49.
Article16. Darby IB, Hodge PJ, Riggio MP, Kinane DF. Clinical and microbiological effect of scaling and root planing in smoker and non-smoker chronic and aggressive periodontitis patients. J Clin Periodontol. 2005; 32:200–206.
Article17. Hughes FJ, Syed M, Koshy B, Marinho V, Bostanci N, McKay IJ, et al. Prognostic factors in the treatment of generalized aggressive periodontitis: I. Clinical features and initial outcome. J Clin Periodontol. 2006; 33:663–670.
Article18. Yek EC, Cintan S, Topcuoglu N, Kulekci G, Issever H, Kantarci A. Efficacy of amoxicillin and metronidazole combination for the management of generalized aggressive periodontitis. J Periodontol. 2010; 81:964–974.
Article19. Guerrero A, Griffiths GS, Nibali L, Suvan J, Moles DR, Laurell L, et al. Adjunctive benefits of systemic amoxicillin and metronidazole in non-surgical treatment of generalized aggressive periodontitis: a randomized placebo-controlled clinical trial. J Clin Periodontol. 2005; 32:1096–1107.20. Kaner D, Bernimoulin JP, Hopfenmuller W, Kleber BM, Friedmann A. Controlled-delivery chlorhexidine chip versus amoxicillin/metronidazole as adjunctive antimicrobial therapy for generalized aggressive periodontitis: a randomized controlled clinical trial. J Clin Periodontol. 2007; 34:880–891.21. Mestnik MJ, Feres M, Figueiredo LC, Duarte PM, Lira EA, Faveri M. Short-term benefits of the adjunctive use of metronidazole plus amoxicillin in the microbial profile and in the clinical parameters of subjects with generalized aggressive periodontitis. J Clin Periodontol. 2010; 37:353–365.22. Baltacioglu E, Aslan M, Sarac O, Saybak A, Yuva P. Analysis of clinical results of systemic antimicrobials combined with nonsurgical periodontal treatment for generalized aggressive periodontitis: a pilot study. J Can Dent Assoc. 2011; 77:b97.23. Wennstrom A, Wennstrom J, Lindhe J. Healing following surgical and non-surgical treatment of juvenile periodontitis: a 5-year longitudinal study. J Clin Periodontol. 1986; 13:869–882.
Article24. Machtei EE, Cho MI, Dunford R, Norderyd J, Zambon JJ, Genco RJ. Clinical, microbiological, and histological factors which influence the success of regenerative periodontal therapy. J Periodontol. 1994; 65:154–161.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical case report on treatment of generalized aggressive periodontitis
- Full mouth fixed implant rehabilitation in a patient with generalized aggressive periodontitis
- The clinical assessment of aggressive periodontitis patients
- Diabetes and Periodontal Disease
- Efficacy of electrical neuromuscular stimulation in the treatment of chronic periodontitis
