Impact of scaling and root planing on C-reactive protein levels in gingival crevicular fluid and serum in chronic periodontitis patients with or without diabetes mellitus
- Affiliations
-
- 1Department of Periodontology, Saraswati Dental College & Hospital, Lucknow, India. doc_vivek76@yahoo.co.in
- 2Department of Periodontology, Rama Dental College Hospital & Research Centre, Kanpur, India.
- 3Kshitiz Medical & Diagnostic Clinic, Lucknow, India.
- KMID: 2212009
- DOI: http://doi.org/10.5051/jpis.2014.44.4.158
Abstract
- PURPOSE
The present study was conducted to evaluate the impact of scaling and root planing (SRP) on the C-reactive protein (CRP) levels of gingival crevicular fluid (GCF) and serum in chronic periodontitis patients with type 2 diabetes mellitus (T2DM-CP) or without type 2 diabetes mellitus (NDM-CP).
METHODS
Forty-eight human participants were divided into two groups: an experimental (T2DM-CP) group (group I, n=24) comprising chronic periodontitis patients with random blood sugar > or =200 mg/dL and type 2 diabetes mellitus, and control (NDM-CP) group (group II, n=24) of those with chronic periodontitis and random blood sugar <200 without T2DM for the study. All subjects underwent nonsurgical periodontal therapy (NSPT) including complete SRP and subgingival debridement. Periodontal health parameters, plaque index (PI), gingival index (GI), probing pocket depth (PPD), clinical attachment level (CAL), GCF volume (GCF vol), GCF-CRP, random blood glucose (RBS), glycated hemoglobin, and systemic inflammatory markers, serum CRP, total leukocyte count (TLC), neutrophil count (Neutr) and lymphocyte count (Lymph), were evaluated at baseline, 1 month, and 3 months after SRP.
RESULTS
NSPT resulted in statistically significant improvement in periodontal health parameters (PI, GI, PPD, CAL, GCF vol), CRP levels in serum as well as GCF of both groups I and II. The mean improvement in periodontal health parameters (PI, GI, PPD, CAL, GCF vol), CRP levels in serum and GCF was greater in group I than group II after NSPT. There was nonsignificant increase in GCF-CRP, TLC, Lymph, and RBS, and a significant increase in Neutr and Serum CRP in group II at 1 month. The Serum CRP level of 20 out of 24 group II patients had also increased at 1 month.
CONCLUSIONS
The CRP levels in both GCF and serum were higher in T2DM-CP patients than in NDM-CP patients. Although there was a significant improvement in both the groups, greater improvement was observed in both GCF and serum samples of T2DM-CP patients.
MeSH Terms
Figure
-

Figure 1 Gingival crevicular fluid C-reactive protein (GCF-CRP) analysis: collection of GCF sample at baseline (A), 1 month (B), and 3 months (C) after scaling and root planing (D) high sensitivity C-reactive protein (CRP) enzyme-linked immunosorbent assay kit (Biotron Diagnostic, Hemet, California, USA) reagents (E) antibody coated microtitre wells (F) standard solutions (G) GCF sample in plastic vial (H) CRP sample diluents (I) retrieval of CRP sample diluents (J).
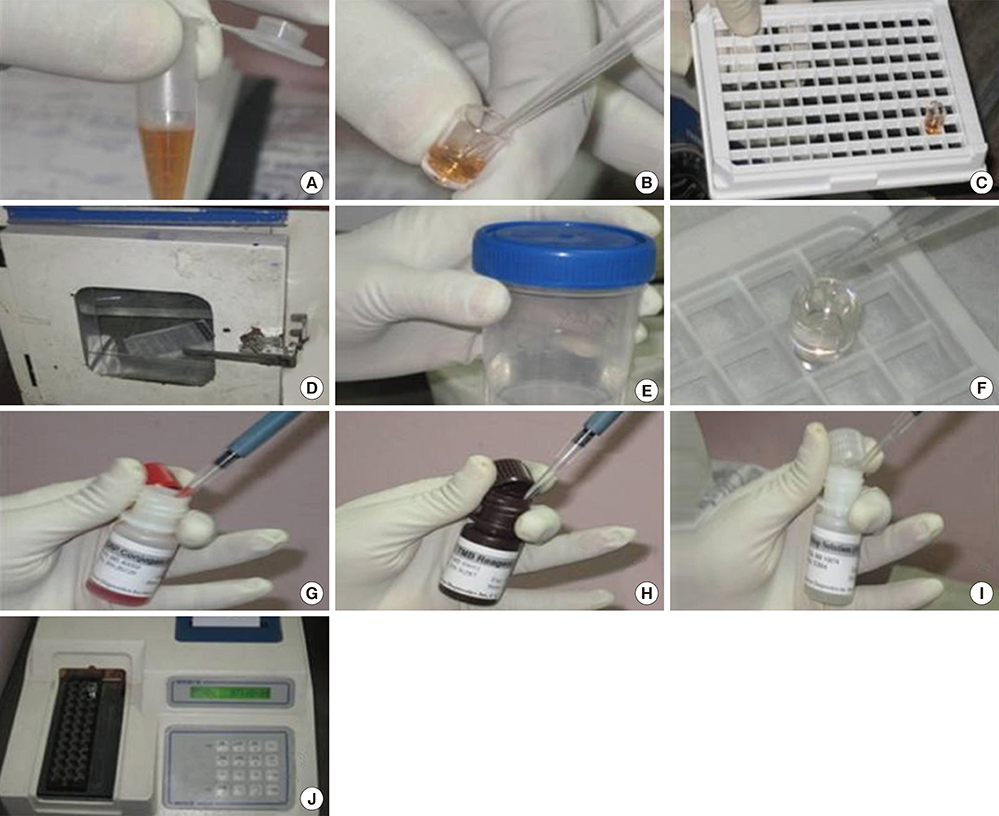
Figure 2 Gingival crevicular fluid C-reactive protein (GCF-CRP) analysis addition of CRP sample diluents to plastic vial containing GCF sample (A) addition of solution in the microtitre well (B) microtitre well in the microtitre plate (C) sample kit in incubator (D) distilled water (E) addition of distilled water in microtitre well (F) retrieval of CRP conjugate (G) retrieval of tetramethylbenzidine reagent (H) retrieval of stop solution (I) microtitre well kept in enzyme-linked immunosorbent assay reader (J).
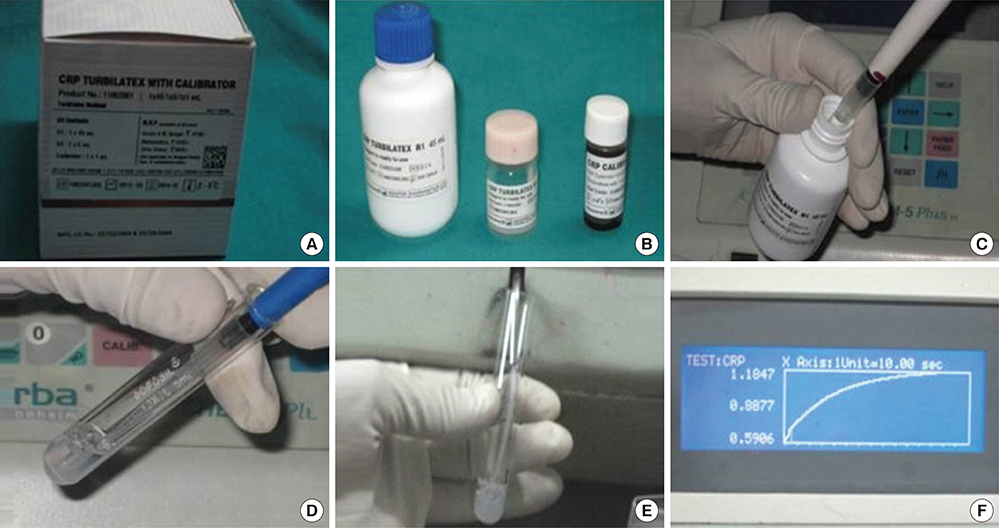
Figure 3 Serum C-reactive protein (CRP) estimation CRP Turbilatex kit (A) reagents (B) reagent R1 in auto-pipette (C) reagent R1 added to test tube containing sample (D) contents in test tube aspirated in semi-auto-analyzer (E) readings with graph in semi-auto-analyzer (F).
Reference
-
1. D'Aiuto F, Parkar M, Andreou G, Brett PM, Ready D, Tonetti MS. Periodontitis and atherogenesis: causal association or simple coincidence? J Clin Periodontol. 2004; 31:402–411.2. Danesh J, Whincup P, Walker M, Lennon L, Thomson A, Appleby P, et al. Low grade inflammation and coronary heart disease: prospective study and up+dated meta-analyses. BMJ. 2000; 321:199–204.
Article3. Galli C, Passeri G, Macaluso GM. FoxOs, Wnts and oxidative stress-induced bone loss: new players in the periodontitis arena? J Periodontal Res. 2011; 46:397–406.
Article4. D'Aiuto F, Nibali L, Parkar M, Suvan J, Tonetti MS. Short-term effects of intensive periodontal therapy on serum inflammatory markers and cholesterol. J Dent Res. 2005; 84:269–273.5. D'Aiuto F, Orlandi M, Gunsolley JC. Evidence that periodontal treatment improves biomarkers and CVD outcomes. J Periodontol. 2013; 84:4 Suppl. S85–S105.6. Pitiphat W, Savetsilp W, Wara-Aswapati N. C-reactive protein associated with periodontitis in a Thai population. J Clin Periodontol. 2008; 35:120–125.
Article7. Pradeep AR, Agarwal E, Bajaj P, Rao NS. 4-Hydroxy-2-nonenal, an oxidative stress marker in crevicular fluid and serum in type 2 diabetes with chronic periodontitis. Contemp Clin Dent. 2013; 4:281–285.
Article8. Evans JL, Goldfine ID, Maddux BA, Grodsky GM. Oxidative stress and stress-activated signaling pathways: a unifying hypothesis of type 2 diabetes. Endocr Rev. 2002; 23:599–622.
Article9. Loe H. Periodontal disease: the sixth complication of diabetes mellitus. Diabetes Care. 1993; 16:329–334.
Article10. Allen EM, Matthews JB, O'Halloran DJ, Griffiths HR, Chapple IL. Oxidative and inflammatory status in Type 2 diabetes patients with periodontitis. J Clin Periodontol. 2011; 38:894–901.
Article11. Losche W, Karapetow F, Pohl A, Pohl C, Kocher T. Plasma lipid and blood glucose levels in patients with destructive periodontal disease. J Clin Periodontol. 2000; 27:537–541.
Article12. Ellen EM, Chapple IL. The relationship between periodontitis and glycaemic control in type 2 diabetes. Eur Endocrinol. 2012; 8:89–93.
Article13. Iacopino AM, Cutler CW. Pathophysiological relationships between periodontitis and systemic disease: recent concepts involving serum lipids. J Periodontol. 2000; 71:1375–1384.
Article14. Pradeep AR, Manjunath RG, Kathariya R. Progressive periodontal disease has a simultaneous incremental elevation of gingival crevicular fluid and serum CRP levels. J Invest Clin Dent. 2010; 1:133–138.
Article15. D'Aiuto F, Parkar M, Andreou G, Suvan J, Brett PM, Ready D, et al. Periodontitis and systemic inflammation: control of the local infection isassociated with a reduction in serum inflammatory markers. J Dent Res. 2004; 83:156–160.16. Navarro-Sanchez AB, Faria-Almeida R, Bascones-Martinez A. Effect of non-surgical periodontal therapy on clinical and immunological response and glycaemic control in type 2 diabetic patients with moderate periodontitis. J Clin Periodontol. 2007; 34:835–843.
Article17. D'Aiuto F, Nibali L, Parkar M, Patel K, Suvan J, Donos N. Oxidative stress, systemic inflammation, and severe periodontitis. J Dent Res. 2010; 89:1241–1246.18. Silness J, Loe H. Periodontal disease in pregnancy. 3. Response to local treatment. Acta Odontol Scand. 1966; 24:747–759.19. Loe H, Silness J. Periodontal disease in pregnancy: I. prevalence and severity. Acta Odontol Scand. 1963; 21:533–551.
Article20. Martin SS, Blaha MJ, Elshazly MB, Brinton EA, Toth PP, McEvoy JW, et al. Friedewald-estimated versus directly measured low-density lipoprotein cholesterol and treatment implications. J Am Coll Cardiol. 2013; 62:732–739.
Article21. Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: a two-way relationship. Ann Periodontol. 1998; 3:51–61.
Article22. Chen L, Luo G, Xuan D, Wei B, Liu F, Li J, et al. Effects of non-surgical periodontal treatment on clinical response, serum inflammatory parameters, and metabolic control in patients with type 2 diabetes: a randomized study. J Periodontol. 2012; 83:435–443.
Article23. Kalra N, Pradeep AR, Priyanka N, Kumari M. Association of stem cell factor and high-sensitivity C reactive protein concentrations in crevicular fluid and serum in patients with chronic periodontitis with and without type 2 diabetes. J Oral Sci. 2013; 55:57–62.
Article24. Kardesler L, Buduneli N, Cetinkalp S, Kinane DF. Adipokines and inflammatory mediators after initial periodontal treatment in patients with type 2 diabetes and chronic periodontitis. J Periodontol. 2010; 81:24–33.
Article25. Tuter G, Serdar M, Kurtis B, Walker SG, Atak A, Toyman U, et al. Effects of scaling and root planing and subantimicrobial dose doxycycline on gingival crevicular fluid levels of matrix metalloproteinase-8, -13 and serum levels of HsCRP in patients with chronic periodontitis. J Periodontol. 2010; 81:1132–1139.
Article26. D'Aiuto F, Parkar M, Tonetti MS. Acute effects of periodontal therapy on bio-markers of vascular health. J Clin Periodontol. 2007; 34:124–129.27. Megson E, Fitzsimmons T, Dharmapatni K, Bartold PM. C-reactive protein in gingival crevicular fluid may be indicative of systemic inflammation. J Clin Periodontol. 2010; 37:797–804.
Article28. D'Aiuto F, Parkar M, Nibali L, Suvan J, Lessem J, Tonetti MS. Periodontal infections cause changes in traditional and novel cardiovascular risk factors: results from a randomized controlled clinical trial. Am Heart J. 2006; 151:977–984.29. Tonetti MS, D'Aiuto F, Nibali L, Donald A, Storry C, Parkar M, et al. Treatment of periodontitis and endothelial function. N Engl J Med. 2007; 356:911–920.
Article30. Lalla E, Kaplan S, Yang J, Roth GA, Papapanou PN, Greenberg S. Effects of periodontal therapy on serum C-reactive protein, sE-selectin, and tumor necrosis factor-alpha secretion by peripheral blood-derived macrophages in diabetes: a pilot study. J Periodontal Res. 2007; 42:274–282.
Article31. Barzilay JI, Abraham L, Heckbert SR, Cushman M, Kuller LH, Resnick HE, et al. The relation of markers of inflammation to the development of glucose disorders in the elderly: the Cardiovascular Health Study. Diabetes. 2001; 50:2384–2389.
Article32. Chen L, Wei B, Li J, Liu F, Xuan D, Xie B, et al. Association of periodontal parameters with metabolic level and systemic inflammatory markers in patients with type 2 diabetes. J Periodontol. 2010; 81:364–371.
Article33. Kamil W, Al Habashneh R, Khader Y, Al Bayati L, Taani D. Effects of nonsurgical periodontal therapy on C-reactive protein and serum lipids in Jordanian adults with advanced periodontitis. J Periodontal Res. 2011; 46:616–621.
Article34. Ide M, McPartlin D, Coward PY, Crook M, Lumb P, Wilson RF. Effect of treatment of chronic periodontitis on levels of serum markers of acute-phase inflammatory and vascular responses. J Clin Periodontol. 2003; 30:334–340.
Article35. Yamazaki K, Honda T, Oda T, Ueki-Maruyama K, Nakajima T, Yoshie H, et al. Effect of periodontal treatment on the C-reactive protein and proinflammatory cytokine levels in Japanese periodontitis patients. J Periodontal Res. 2005; 40:53–58.
Article36. Fredriksson MI, Gustafsson AK, Bergström KG, Asman BE. Constitutionally hyperreactive neutrophils in periodontitis. J Periodontol. 2003; 74:219–224.
Article37. Sun WL, Chen LL, Zhang SZ, Wu YM, Ren YZ, Qin GM. Inflammatory cytokines, adiponectin, insulin resistance and metabolic control after periodontal intervention in patients with type 2 diabetes and chronic periodontitis. Intern Med. 2011; 50:1569–1574.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of scaling and root planing with or without a local drug delivery system on the gingival crevicular fluid leptin level in chronic periodontitis patients: a clinico-biochemical study
- Clinical and Microbiological Study about Efficacy of Air-polishing and Scaling and Root-planing
- The effects of low dose doxycycline regimen on gingival crevicular fluid enzyme actmty of diabetic patients with periodontitis and adult periodontitis patients
- Effect of scaling and root planing on the expression of anti-inflammatory cytokines (IL-4, IL-9, IL-10, and IL-13)in the gingival crevicular fluid of electronic cigarette users andnon-smokers with moderate chronic periodontitis
- Effect of scaling and root planing combined with systemic doxycycline therapy on glycemic control in diabetes mellitus subjects with chronic generalized periodontitis: a clinical study
